Potrebbero piacerti anche
- Surgery For Pelvic Organ Prolapse: The American College of Obstetricians and GynecologistsDocumento4 pagineSurgery For Pelvic Organ Prolapse: The American College of Obstetricians and GynecologistsKartika FitriNessuna valutazione finora
- FeverDocumento39 pagineFeverKartika FitriNessuna valutazione finora
- American Academy of Pediatrics: Olicy TatementDocumento5 pagineAmerican Academy of Pediatrics: Olicy TatementKartika FitriNessuna valutazione finora
- SampleSize TAScott Handout PDFDocumento12 pagineSampleSize TAScott Handout PDFKartika FitriNessuna valutazione finora
- Cirrhosis and Its Complications: Dr. P. Dienhart, M.D (Gastroenterology) DR - Padma Poddutoori (PGY3, I.M)Documento21 pagineCirrhosis and Its Complications: Dr. P. Dienhart, M.D (Gastroenterology) DR - Padma Poddutoori (PGY3, I.M)Kartika FitriNessuna valutazione finora
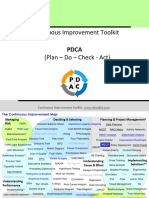
- Continuous Improvement ToolkitDocumento16 pagineContinuous Improvement ToolkitKartika Fitri100% (1)
- Mental Illness Questionnaire Nov 2001Documento6 pagineMental Illness Questionnaire Nov 2001Kartika FitriNessuna valutazione finora
- Gizi Seimbang and Adequate NutritionDocumento7 pagineGizi Seimbang and Adequate NutritionKartika FitriNessuna valutazione finora
- s15 Miller Chap 8b LectureDocumento19 pagines15 Miller Chap 8b LectureKartika FitriNessuna valutazione finora
- Pre-Operative AssessmentDocumento33 paginePre-Operative AssessmentKartika FitriNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Theories of EmotionDocumento11 pagineTheories of EmotionNoman ANessuna valutazione finora
- Science 7 Las 1Documento4 pagineScience 7 Las 1Paris AtiaganNessuna valutazione finora
- RMK Akl 2 Bab 5Documento2 pagineRMK Akl 2 Bab 5ElineNessuna valutazione finora
- Understanding The School Curriculum Close Encounter With The School Curriculum SPARK Your InterestDocumento12 pagineUnderstanding The School Curriculum Close Encounter With The School Curriculum SPARK Your InterestJoshua Lander Soquita CadayonaNessuna valutazione finora
- Permanently End Premature EjaculationDocumento198 paginePermanently End Premature EjaculationZachary Leow100% (5)
- Traverse AdjustmentDocumento22 pagineTraverse AdjustmenthabteNessuna valutazione finora
- Account StatementDocumento12 pagineAccount StatementbadramostuNessuna valutazione finora
- List of Mines in IndiaDocumento4 pagineList of Mines in IndiaNAMISH MAHAKULNessuna valutazione finora
- Tiny House 2020: Less House, More HomeDocumento11 pagineTiny House 2020: Less House, More HomeVanshika SpeedyNessuna valutazione finora
- Online Book Store System: Bachelor of Computer EngineeringDocumento31 pagineOnline Book Store System: Bachelor of Computer Engineeringkalpesh mayekarNessuna valutazione finora
- CABE Space - A Guide To Producing Park and Green Space Management PlansDocumento48 pagineCABE Space - A Guide To Producing Park and Green Space Management PlansbenconnolleyNessuna valutazione finora
- R WaseemDocumento3 pagineR WaseemWaseem RajaNessuna valutazione finora
- 6.4 Past Simple Affirmative: 0 Called HadDocumento1 pagina6.4 Past Simple Affirmative: 0 Called HadSashkaKoreckajaNessuna valutazione finora
- Islamic Architecture PDFDocumento59 pagineIslamic Architecture PDFHarshi Garg100% (3)
- The Mystery of The Secret RoomDocumento3 pagineThe Mystery of The Secret RoomNur Farhana100% (2)
- Low Steam Cane - Almoiz Industries Road To SuccessDocumento9 pagineLow Steam Cane - Almoiz Industries Road To SuccessArif ShafiNessuna valutazione finora
- Farewell Address WorksheetDocumento3 pagineFarewell Address Worksheetapi-261464658Nessuna valutazione finora
- Case: Iridium LLC: Bhanu - Divya - Harsh - NamitaDocumento9 pagineCase: Iridium LLC: Bhanu - Divya - Harsh - NamitaHarsh AgrawalNessuna valutazione finora
- Cb-3 Mech'l Plans 05.06.22Documento12 pagineCb-3 Mech'l Plans 05.06.22Mark Vincent MoraNessuna valutazione finora
- QinQ Configuration PDFDocumento76 pagineQinQ Configuration PDF_kochalo_100% (1)
- Sustainable Building: Submitted By-Naitik JaiswalDocumento17 pagineSustainable Building: Submitted By-Naitik JaiswalNaitik JaiswalNessuna valutazione finora
- C Programming Bit Bank U-1, U-2Documento17 pagineC Programming Bit Bank U-1, U-2HariahNessuna valutazione finora
- Certified List of Candidates For Congressional and Local Positions For The May 13, 2013 2013 National, Local and Armm ElectionsDocumento2 pagineCertified List of Candidates For Congressional and Local Positions For The May 13, 2013 2013 National, Local and Armm ElectionsSunStar Philippine NewsNessuna valutazione finora
- NHD Process Paper 1Documento2 pagineNHD Process Paper 1api-544229559Nessuna valutazione finora
- Binder1 CARENCRODocumento27 pagineBinder1 CARENCROAddisu TsehayNessuna valutazione finora
- Eastwoods: College of Science and Technology, IncDocumento2 pagineEastwoods: College of Science and Technology, IncMichael AustriaNessuna valutazione finora
- Giant Panda: 1 DescriptionDocumento18 pagineGiant Panda: 1 DescriptionMsKarolyNessuna valutazione finora
- CS101 Solved File For Final Term MCQS 1 To 45 LecturesDocumento130 pagineCS101 Solved File For Final Term MCQS 1 To 45 LecturesHisan Mehmood64% (28)
- College Physics Global 10th Edition Young Solutions ManualDocumento25 pagineCollege Physics Global 10th Edition Young Solutions ManualSaraSmithdgyj100% (57)
- 2406 Final ExamDocumento10 pagine2406 Final ExamChandan GargNessuna valutazione finora