Potrebbero piacerti anche
- East Coast Q3 2014 Letter - Grove of TitansDocumento16 pagineEast Coast Q3 2014 Letter - Grove of TitansCanadianValue100% (1)
- Test Bank For Friedland Relyea Environmental Science For APDocumento13 pagineTest Bank For Friedland Relyea Environmental Science For APFrances WhiteNessuna valutazione finora
- Medical ProtozoologyDocumento6 pagineMedical ProtozoologyRaymund MontoyaNessuna valutazione finora
- TrematodesDocumento9 pagineTrematodesLewis P. SanchezNessuna valutazione finora
- Blood and Tissue NematodesDocumento3 pagineBlood and Tissue Nematodesdotsdy100% (3)
- Parasitology - CestodesDocumento23 pagineParasitology - CestodesJeth Roque GalleneroNessuna valutazione finora
- Parasaitology HelminthDocumento139 pagineParasaitology Helminthkidus asnNessuna valutazione finora
- Cestodes and Trematodes: A Comparison of Tapeworms and FlukesDocumento4 pagineCestodes and Trematodes: A Comparison of Tapeworms and FlukesNatalie EnriquezNessuna valutazione finora
- NematodaDocumento96 pagineNematodaPurplesmilezNessuna valutazione finora
- Cestode NotesDocumento26 pagineCestode NotesJOSEPH NDERITUNessuna valutazione finora
- Blood Tissue NematodesDocumento27 pagineBlood Tissue NematodesAfif Mamen100% (1)
- Leishmaniasis and Trypanosomiasis Parasite Identification QuestionsDocumento39 pagineLeishmaniasis and Trypanosomiasis Parasite Identification QuestionsMonique Eloise GualizaNessuna valutazione finora
- CestodesDocumento86 pagineCestodesPidchayathanakorn Paemika0% (1)
- (QUIZ) NEMATODES (2nd Year BS Medical Technology)Documento2 pagine(QUIZ) NEMATODES (2nd Year BS Medical Technology)avery aerNessuna valutazione finora
- Arthro 1Documento55 pagineArthro 1MenDel Icj IcjiNessuna valutazione finora
- Comprehensive Exam #2 Rationalization: ParasitologyDocumento5 pagineComprehensive Exam #2 Rationalization: ParasitologyJoyceNessuna valutazione finora
- Entamoeba ColiDocumento14 pagineEntamoeba ColiHanisha Erica100% (1)
- Classification, General Characteristics of Parasites and Medically Important ParasitesDocumento30 pagineClassification, General Characteristics of Parasites and Medically Important ParasitesSteph AsideNessuna valutazione finora
- The Ameba ReportingDocumento49 pagineThe Ameba ReportingALLISON PAMITTANNessuna valutazione finora
- Levanthan Short Ans KeyDocumento42 pagineLevanthan Short Ans Keyxyab.varga.swuNessuna valutazione finora
- Trematode Lec QuizDocumento2 pagineTrematode Lec QuizCia Lomh0% (1)
- Para-Transes Prelim Exam - Unit 2Documento20 paginePara-Transes Prelim Exam - Unit 2Aysha AishaNessuna valutazione finora
- Trematodes PDFDocumento46 pagineTrematodes PDFAsnorah SaripNessuna valutazione finora
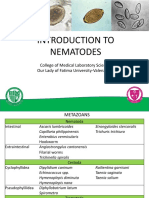
- Introduction To Nematodes: College of Medical Laboratory Science Our Lady of Fatima University-ValenzuelaDocumento29 pagineIntroduction To Nematodes: College of Medical Laboratory Science Our Lady of Fatima University-ValenzuelaMichNessuna valutazione finora
- TrematodesDocumento30 pagineTrematodesJezzah Mae CañeteNessuna valutazione finora
- 2 PARA 3 - AmoebasDocumento8 pagine2 PARA 3 - AmoebasTricia LlorinNessuna valutazione finora
- TREMATODESDocumento31 pagineTREMATODESKen Mark ConcepcionNessuna valutazione finora
- Parasitology Lecture 11 - AphasmidsDocumento4 pagineParasitology Lecture 11 - Aphasmidsmiguel cuevasNessuna valutazione finora
- Cestode SDocumento79 pagineCestode SVincent Manganaan67% (3)
- Clinical Parasitology Microscope GuideDocumento4 pagineClinical Parasitology Microscope GuideLyka ReyesNessuna valutazione finora
- Cestodes and Trematodes - ReviewerDocumento2 pagineCestodes and Trematodes - ReviewerAnna LouisaNessuna valutazione finora
- Loa loa eye wormDocumento12 pagineLoa loa eye wormRajesh Kumar AsunalaNessuna valutazione finora
- Blood Tissue and FlagellatesDocumento15 pagineBlood Tissue and FlagellatesHughNessuna valutazione finora
- Trematode Characteristics and Life CyclesDocumento2 pagineTrematode Characteristics and Life CyclesGougle MuteNessuna valutazione finora
- CESTODES: KEY CHARACTERISTICS AND CLASSIFICATIONDocumento86 pagineCESTODES: KEY CHARACTERISTICS AND CLASSIFICATIONKendon D. TajanlangitNessuna valutazione finora
- TogaviridaeDocumento60 pagineTogaviridae2013SecB50% (2)
- Accurate Diagnosis of Parasitic Infections Is Important To Decrease The Prevalence andDocumento4 pagineAccurate Diagnosis of Parasitic Infections Is Important To Decrease The Prevalence andManulat VicaiiNessuna valutazione finora
- Classification of ProtozoaDocumento1 paginaClassification of ProtozoaSalil ShauNessuna valutazione finora
- Lecture Notes BacteriologyDocumento133 pagineLecture Notes BacteriologyLovely B. AlipatNessuna valutazione finora
- Malaria Plasmodium SPP WPDocumento5 pagineMalaria Plasmodium SPP WPPerlie CNessuna valutazione finora
- Common Parasitic Infections - Life Cycles and TreatmentsDocumento7 pagineCommon Parasitic Infections - Life Cycles and TreatmentsAj MillanNessuna valutazione finora
- NematodesDocumento4 pagineNematodesPrincess Shaina CanapeNessuna valutazione finora
- Morpholofy of MoDocumento44 pagineMorpholofy of MoPathumavathy RamanathanNessuna valutazione finora
- Cestode SDocumento38 pagineCestode SJang JangNessuna valutazione finora
- HookwormDocumento10 pagineHookwormAmelyalesmanaNessuna valutazione finora
- Parasitic Infection in GI TractDocumento123 pagineParasitic Infection in GI TractUtami HandayaniNessuna valutazione finora
- Introduction To Medical Parasitology Prepared By: Geraldine P. PulidoDocumento26 pagineIntroduction To Medical Parasitology Prepared By: Geraldine P. PulidoMark Reynie Renz SilvaNessuna valutazione finora
- Parasitology - Lec - FinalDocumento69 pagineParasitology - Lec - FinalJannah Monaliza BambaNessuna valutazione finora
- Parasitology Table ProtozoaDocumento10 pagineParasitology Table ProtozoaMae Rose Charlene MendozaNessuna valutazione finora
- Introduction To Diagnostic Parasitology: (Specimen Collection and Handling)Documento26 pagineIntroduction To Diagnostic Parasitology: (Specimen Collection and Handling)RIC JOSEPH PONCIANONessuna valutazione finora
- Introduction To Cestodes and Minor CestodesDocumento8 pagineIntroduction To Cestodes and Minor CestodesJustin TayabanNessuna valutazione finora
- Trichomoniasis: T. Vaginalis Is A Parasitic Protozoan, and The Taxonomic Position Is Based On The ClassificationDocumento15 pagineTrichomoniasis: T. Vaginalis Is A Parasitic Protozoan, and The Taxonomic Position Is Based On The Classificationrave robNessuna valutazione finora
- Cestodes 2020Documento10 pagineCestodes 2020CDNessuna valutazione finora
- Coccidia 10 - 11Documento40 pagineCoccidia 10 - 11microperadeniya100% (1)
- Nematodes and Their Life CyclesDocumento18 pagineNematodes and Their Life Cyclesnicole syNessuna valutazione finora
- CMB Lab Oral ReportDocumento17 pagineCMB Lab Oral ReportKai ChenNessuna valutazione finora
- Ex 2 CmblabDocumento31 pagineEx 2 CmblabrexartoozNessuna valutazione finora
- ReviewersDocumento1 paginaReviewersRalph Renon CasamayorNessuna valutazione finora
- PARASITOLOGY NotesDocumento36 paginePARASITOLOGY NotesTumabang DivineNessuna valutazione finora
- TRICHINELLADocumento27 pagineTRICHINELLARajkishor YadavNessuna valutazione finora
- Tri Chin EllaDocumento2 pagineTri Chin EllaPrincess MhnNessuna valutazione finora
- Trichinella Spiralis Parasite: Symptoms, Life Cycle & TreatmentDocumento15 pagineTrichinella Spiralis Parasite: Symptoms, Life Cycle & TreatmentBenjamin DanielNessuna valutazione finora
- RX 3 and 4 1Documento1 paginaRX 3 and 4 1Vincent ManganaanNessuna valutazione finora
- Pope Francis in The PhilippinesDocumento4 paginePope Francis in The PhilippinesVincent ManganaanNessuna valutazione finora
- Incompatibilities RWFDocumento12 pagineIncompatibilities RWFVincent ManganaanNessuna valutazione finora
- Incompatibilities RWFDocumento12 pagineIncompatibilities RWFVincent ManganaanNessuna valutazione finora
- Lipids: StructureDocumento42 pagineLipids: Structurecream oNessuna valutazione finora
- Revised S A Syllabus 2017-2018Documento12 pagineRevised S A Syllabus 2017-2018Vincent ManganaanNessuna valutazione finora
- Shigellosis Written ReportDocumento4 pagineShigellosis Written ReportVincent ManganaanNessuna valutazione finora
- Unit 1: Introduction: Theoretical Perspectives & Contemporary Issues On Dispensing & Patient Medication CounselingDocumento14 pagineUnit 1: Introduction: Theoretical Perspectives & Contemporary Issues On Dispensing & Patient Medication CounselingVincent ManganaanNessuna valutazione finora
- Oral Rehydration SaltDocumento3 pagineOral Rehydration SaltVincent ManganaanNessuna valutazione finora
- Cestode SDocumento79 pagineCestode SVincent Manganaan67% (3)
- Pope Francis in The PhilippinesDocumento4 paginePope Francis in The PhilippinesVincent ManganaanNessuna valutazione finora
- EatDocumento1 paginaEatVincent ManganaanNessuna valutazione finora
- Biology Nmat @Documento6 pagineBiology Nmat @Ma. Ellah Patricia M. GutierrezNessuna valutazione finora
- Intestinal NematodesDocumento88 pagineIntestinal NematodesVincent Manganaan100% (1)
- Thermal Conductivity and Linear ExpansionDocumento21 pagineThermal Conductivity and Linear ExpansionVincent ManganaanNessuna valutazione finora
- Heat Lec2 MethodDocumento15 pagineHeat Lec2 MethodVincent ManganaanNessuna valutazione finora
- FinalDocumento13 pagineFinalVincent ManganaanNessuna valutazione finora
- Carbohydrates Postlab2 1Documento37 pagineCarbohydrates Postlab2 1Vincent ManganaanNessuna valutazione finora
- Lipids 2Documento30 pagineLipids 2Vincent ManganaanNessuna valutazione finora
- Fusion in CalorimetryDocumento6 pagineFusion in CalorimetryVincent ManganaanNessuna valutazione finora
- Carbohydrate Postlab1 1Documento33 pagineCarbohydrate Postlab1 1Vincent ManganaanNessuna valutazione finora
- Chapter 12 - SuppositoriesDocumento5 pagineChapter 12 - SuppositoriesAli Uy100% (1)
- EndocrineDocumento83 pagineEndocrineVincent ManganaanNessuna valutazione finora
- Blood PDFDocumento55 pagineBlood PDFlorrainebarandonNessuna valutazione finora
- Blood VesselsDocumento86 pagineBlood VesselsVincent ManganaanNessuna valutazione finora
- Isolation and Characterization of CarbohDocumento6 pagineIsolation and Characterization of CarbohVincent ManganaanNessuna valutazione finora
- Physics Exp 6 IntroductionDocumento1 paginaPhysics Exp 6 IntroductionVincent ManganaanNessuna valutazione finora
- Subtotal and Total Thyroidectomy: AuthorDocumento10 pagineSubtotal and Total Thyroidectomy: AuthorAgustina TambingNessuna valutazione finora
- B VIDAS T4 enDocumento7 pagineB VIDAS T4 enInn MironNessuna valutazione finora
- Year 12 Biology - CH 10 Genes and DNADocumento4 pagineYear 12 Biology - CH 10 Genes and DNAJessica100% (1)
- Snorks Udl Lesson Plan-1Documento4 pagineSnorks Udl Lesson Plan-1api-253110466Nessuna valutazione finora
- What Is The Lifespan of A Glofish - Google SearchDocumento1 paginaWhat Is The Lifespan of A Glofish - Google SearchaddisoncmooreNessuna valutazione finora
- Lambda Cyhalothrin Ecm WaterDocumento13 pagineLambda Cyhalothrin Ecm WaterspveceNessuna valutazione finora
- SP4 Memes - UmaliDocumento6 pagineSP4 Memes - UmaliSheryl Anne Benigno UmaliNessuna valutazione finora
- Wbi15 01 Que 20231024Documento36 pagineWbi15 01 Que 20231024MuqtasidNessuna valutazione finora
- Structure of Crystals WebexDocumento22 pagineStructure of Crystals WebexmareasanthaNessuna valutazione finora
- Interpretation of Histograms and Peripheral Smear FindingsDocumento5 pagineInterpretation of Histograms and Peripheral Smear FindingsrezqiNessuna valutazione finora
- Ted Talk Reflection 1Documento3 pagineTed Talk Reflection 1api-242138662Nessuna valutazione finora
- Sphaerica and Oscillatoria AgardhiiDocumento17 pagineSphaerica and Oscillatoria AgardhiiMhemeydha Luphe YudhaNessuna valutazione finora
- 2nd PERIODICAL EXAMDocumento18 pagine2nd PERIODICAL EXAMJhuanna Marie CabalteraNessuna valutazione finora
- AnswersDocumento36 pagineAnswersNaina Garg100% (1)
- B. Pharm Syllabus 2014 Submitted To RGUHSDocumento130 pagineB. Pharm Syllabus 2014 Submitted To RGUHSIbrahim GatarNessuna valutazione finora
- The Phenomenon of ManDocumento12 pagineThe Phenomenon of ManPaul Schumann83% (6)
- Sticky Trap Monitoring of Insect Pests: Steve H. DreistadtDocumento8 pagineSticky Trap Monitoring of Insect Pests: Steve H. DreistadtBryan AbarcaNessuna valutazione finora
- Microb Monitor 2 Instructions UseDocumento5 pagineMicrob Monitor 2 Instructions UseArluky NovandyNessuna valutazione finora
- Pforams@Mikrotax - Globigerinoides ConglobatusDocumento2 paginePforams@Mikrotax - Globigerinoides ConglobatusAhmad Lumban GaolNessuna valutazione finora
- English 2 Class 02Documento23 pagineEnglish 2 Class 02Bill YohanesNessuna valutazione finora
- 4.1.3 - State of The Australian Environment - StudentDocumento5 pagine4.1.3 - State of The Australian Environment - StudentMatthew Pringle100% (1)
- Western Mindanao State University College of Agriculture Zamboanga CityDocumento7 pagineWestern Mindanao State University College of Agriculture Zamboanga CityJolina bacusNessuna valutazione finora
- QC ABO RH BloodDocumento62 pagineQC ABO RH BloodrhoderickNessuna valutazione finora
- Therapy PolarityDocumento37 pagineTherapy PolarityNaina RavahitrarivoNessuna valutazione finora
- MlistDocumento13 pagineMlistSumanth MopideviNessuna valutazione finora
- Updated WorksheetDocumento5 pagineUpdated WorksheetJohn Ramer Lazarte InocencioNessuna valutazione finora
- Kung Et Al. (2018)Documento14 pagineKung Et Al. (2018)Henry Daniel Ruiz AlbaNessuna valutazione finora
- Trigger Point Therapy Routine For TMJ Massage Techniques To Unlock Your TMJ PDFDocumento49 pagineTrigger Point Therapy Routine For TMJ Massage Techniques To Unlock Your TMJ PDFMilijana D. Delević40% (5)