Potrebbero piacerti anche
- Transfer Factors: Properties, Mechanism of Action and Its Clinical ApplicationsDa EverandTransfer Factors: Properties, Mechanism of Action and Its Clinical ApplicationsNessuna valutazione finora
- Human Immuno Deficiency VirusDocumento15 pagineHuman Immuno Deficiency VirusDayana PrasanthNessuna valutazione finora
- Chapter 6 - Immune Diseases (Part II) (Robbins and Cotran Pathologic Basis of Disease)Documento3 pagineChapter 6 - Immune Diseases (Part II) (Robbins and Cotran Pathologic Basis of Disease)Ernie G. Bautista II, RN, MD100% (5)
- Is HivDocumento50 pagineIs HivRodriguez, Jhe-ann M.Nessuna valutazione finora
- Dengue Fever With Hepatitis E and Hepatitis A Infection PDFDocumento2 pagineDengue Fever With Hepatitis E and Hepatitis A Infection PDFAMENDBENessuna valutazione finora
- AIDS Project (Bios 328)Documento36 pagineAIDS Project (Bios 328)tammdocNessuna valutazione finora
- Reviewofprimary ImmunodeficiencydiseasesDocumento58 pagineReviewofprimary Immunodeficiencydiseasespriti adsulNessuna valutazione finora
- Acquired Immuno-Deficiency Syndrome (AIDS) : Savitha R S JSSCP, MysoreDocumento41 pagineAcquired Immuno-Deficiency Syndrome (AIDS) : Savitha R S JSSCP, MysorerathanNessuna valutazione finora
- HivDocumento49 pagineHivPriyanka GuptaNessuna valutazione finora
- 1 s2.0 S0749070421000981 MainDocumento11 pagine1 s2.0 S0749070421000981 MainEliseu AmaralNessuna valutazione finora
- Aids With CMVDocumento8 pagineAids With CMVIchunx MelissaNessuna valutazione finora
- Lecture 1moninfect ImmuDocumento50 pagineLecture 1moninfect ImmuFrancisco HenriquezNessuna valutazione finora
- Summary of HIV/AIDSDocumento5 pagineSummary of HIV/AIDSbibiMh100% (1)
- Immuno NotesDocumento9 pagineImmuno NotesMoe HussainNessuna valutazione finora
- Immunodeficiencies: Causes, Diagnosis and TreatmentDocumento10 pagineImmunodeficiencies: Causes, Diagnosis and TreatmentAhmed Goma'aNessuna valutazione finora
- Digging Up The Bones - MicrobiologyDocumento31 pagineDigging Up The Bones - MicrobiologyMossa Di Base100% (1)
- Google 5Documento35 pagineGoogle 5VizhiNessuna valutazione finora
- 58 19Documento10 pagine58 19Alberto RamirezNessuna valutazione finora
- Autoimmune Variant PTPN22 C1858T Is Associated With Impaired Responses To in Uenza VaccinationDocumento10 pagineAutoimmune Variant PTPN22 C1858T Is Associated With Impaired Responses To in Uenza VaccinationSuci SetiawatiNessuna valutazione finora
- Herpes Viruses: Viruses Causing Latent InfectionsDocumento96 pagineHerpes Viruses: Viruses Causing Latent InfectionsSolustNessuna valutazione finora
- Biomarkers in SepsisDocumento33 pagineBiomarkers in SepsisAnjana KsNessuna valutazione finora
- Nri1201 Hiv PosterDocumento1 paginaNri1201 Hiv Posteranirbanmanna88320100% (1)
- Human Lentiviral Gene Therapy Restores1111Documento11 pagineHuman Lentiviral Gene Therapy Restores1111Cuenta ExtraNessuna valutazione finora
- Auto Immune DiseasesDocumento18 pagineAuto Immune DiseasesNareshNessuna valutazione finora
- Hiv/Aids Seminar: September, 2011Documento45 pagineHiv/Aids Seminar: September, 2011Diress MollaNessuna valutazione finora
- X-Linked Hyper-Igm Syndrome With Cd40Lg Mutation: Two Case Reports and Literature Review in Taiwanese PatientsDocumento6 pagineX-Linked Hyper-Igm Syndrome With Cd40Lg Mutation: Two Case Reports and Literature Review in Taiwanese PatientsNutriologo Luis Garcia CampechanoNessuna valutazione finora
- Immunology 2Documento30 pagineImmunology 2ukashazam19Nessuna valutazione finora
- Epstein-Barr Virus Super FinalDocumento6 pagineEpstein-Barr Virus Super FinalStill DollNessuna valutazione finora
- DR - Dr.efrida Warganegara, M.Kes., SP - MKDocumento30 pagineDR - Dr.efrida Warganegara, M.Kes., SP - MKDedy SantosoNessuna valutazione finora
- Immunology Uworld Notes (Step 1)Documento12 pagineImmunology Uworld Notes (Step 1)Burkitt's LymphomaNessuna valutazione finora
- Managing Infections in Immunocompromised PatientsDocumento26 pagineManaging Infections in Immunocompromised Patientsmmkavitha98Nessuna valutazione finora
- HIV Notes (Clinical Virology) MR - ManigaDocumento31 pagineHIV Notes (Clinical Virology) MR - ManigaDaniel OkakaNessuna valutazione finora
- Innate Immunity Cells and Their Role in Nonadaptive Immune ResponsesDocumento13 pagineInnate Immunity Cells and Their Role in Nonadaptive Immune ResponsesShaz ChindhyNessuna valutazione finora
- Lec 6Documento32 pagineLec 6Ghadi AbdalazizNessuna valutazione finora
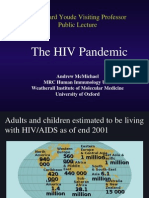
- The HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureDocumento50 pagineThe HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureSanthosh SubramanianNessuna valutazione finora
- ITV Generates Specific Anti-HIV AntibodiesDocumento18 pagineITV Generates Specific Anti-HIV AntibodiesMutiaraa Sarii DewiiNessuna valutazione finora
- HIV&HepatitisDocumento100 pagineHIV&HepatitisRaja RuzannaNessuna valutazione finora
- (17b) RetroviridaeDocumento50 pagine(17b) RetroviridaeFarrah BenoitNessuna valutazione finora
- HivDocumento29 pagineHivSUTHAN100% (2)
- Thl/Th2 Profiles Tuberculosis, Proliferation Cytokine of Blood Lymphocytes Mycobacterial AntigensDocumento6 pagineThl/Th2 Profiles Tuberculosis, Proliferation Cytokine of Blood Lymphocytes Mycobacterial AntigensAdolfo Arturo Ccencho VacasNessuna valutazione finora
- MISC - Multisystem Inflammatory Syndrome in in Children (An Unfortunate COVID 19 Aftermath in Children) - DR Akshay P Jadhav MD Pediatrics Fellow PED ICU Fellow Ped EmergencyDocumento62 pagineMISC - Multisystem Inflammatory Syndrome in in Children (An Unfortunate COVID 19 Aftermath in Children) - DR Akshay P Jadhav MD Pediatrics Fellow PED ICU Fellow Ped EmergencyDr Akshay P JadhavNessuna valutazione finora
- Present Status of Anti-Hiv DrugsDocumento7 paginePresent Status of Anti-Hiv Drugsbrijesh1411Nessuna valutazione finora
- Immunology For AiimsDocumento21 pagineImmunology For AiimssureshNessuna valutazione finora
- Classification of Interferons (Ifns) : Interferons and Chemokines Cytokine Receptors/Signaling Adhesion MoleculesDocumento10 pagineClassification of Interferons (Ifns) : Interferons and Chemokines Cytokine Receptors/Signaling Adhesion MoleculesLucas AresNessuna valutazione finora
- Presented By: DR - Biswajeeta Saha (1 Yr PG) Moderator: Dr. N. Sahu, Dept of Pathology, Kims, BBSRDocumento43 paginePresented By: DR - Biswajeeta Saha (1 Yr PG) Moderator: Dr. N. Sahu, Dept of Pathology, Kims, BBSRBiswajeeta SahaNessuna valutazione finora
- General Features of The Immune SystemDocumento6 pagineGeneral Features of The Immune SystemMinerva Bautista RoseteNessuna valutazione finora
- HIV DISEASE - Physiotherapy ClassDocumento32 pagineHIV DISEASE - Physiotherapy ClassPraveen RajNessuna valutazione finora
- Immunology Micro D&R AgamDocumento146 pagineImmunology Micro D&R AgamNirosha Arul100% (1)
- Molecular Virology of HIV and Current Antiviral StrategiesDocumento7 pagineMolecular Virology of HIV and Current Antiviral StrategiesDitha FadhilaNessuna valutazione finora
- Listeria Innocua VGC: Protective Immunity To Listeria Monocytogenes Infection Mediated by Recombinant Harboring The LocusDocumento9 pagineListeria Innocua VGC: Protective Immunity To Listeria Monocytogenes Infection Mediated by Recombinant Harboring The LocuscaballobluemetalNessuna valutazione finora
- Prodia Clinical Laboratory:: 1. Specialty & Research Laboratory Manager, 3. IaccDocumento55 pagineProdia Clinical Laboratory:: 1. Specialty & Research Laboratory Manager, 3. Iaccpraditanovia rengganisNessuna valutazione finora
- Serum Procalcitonin For Differentiating Bacterial Infection From Disease Flares in Patients With Systemic Lupus ErythematosusDocumento29 pagineSerum Procalcitonin For Differentiating Bacterial Infection From Disease Flares in Patients With Systemic Lupus ErythematosusHadi SusilaNessuna valutazione finora
- Clinical ImmunologyDocumento5 pagineClinical ImmunologyiuventasNessuna valutazione finora
- Il28b 2015Documento7 pagineIl28b 2015Hafsa AzizNessuna valutazione finora
- How Do B Cells Produce Antibodies?Documento165 pagineHow Do B Cells Produce Antibodies?Sharmaine TrangiaNessuna valutazione finora
- Immunology For BPTs 2020 - OCR, CompressedDocumento156 pagineImmunology For BPTs 2020 - OCR, CompressedtjelongNessuna valutazione finora
- HIV InfectionDocumento47 pagineHIV InfectionMarwanNessuna valutazione finora
- Immunology and MicrobiologyDocumento91 pagineImmunology and MicrobiologyB.simhachalamNessuna valutazione finora
- GRAFT VS HOST AND TRANSPLANT INFECTIONDocumento44 pagineGRAFT VS HOST AND TRANSPLANT INFECTIONHasna Mirda AmazanNessuna valutazione finora
- Viral Properties and ReplicationDocumento43 pagineViral Properties and ReplicationSarah PavuNessuna valutazione finora
- #Rhabdo Virus#Documento13 pagine#Rhabdo Virus#Sarah PavuNessuna valutazione finora
- Rickettsiaceae &Documento25 pagineRickettsiaceae &Sarah PavuNessuna valutazione finora
- Viral Properties and ReplicationDocumento43 pagineViral Properties and ReplicationSarah PavuNessuna valutazione finora
- #Staphylococcus &#Documento10 pagine#Staphylococcus &#Sarah PavuNessuna valutazione finora
- Adeno Viruses2Documento8 pagineAdeno Viruses2Sarah PavuNessuna valutazione finora
- Pox VirusesDocumento11 paginePox VirusesSarah PavuNessuna valutazione finora
- Herpes VirusDocumento22 pagineHerpes VirusSarah PavuNessuna valutazione finora
- Rhabdo VirusDocumento13 pagineRhabdo VirusSarah PavuNessuna valutazione finora
- Hepatitis VirusDocumento11 pagineHepatitis VirusSarah PavuNessuna valutazione finora
- RetrovirusDocumento11 pagineRetrovirusSarah PavuNessuna valutazione finora
- ##Documento12 pagine##Sarah PavuNessuna valutazione finora
- SPIROCHAETES & MYCOPLASMA: MORPHOLOGY AND PATHOGENESISDocumento28 pagineSPIROCHAETES & MYCOPLASMA: MORPHOLOGY AND PATHOGENESISSarah PavuNessuna valutazione finora
- Normal Microflora of Human BodyDocumento14 pagineNormal Microflora of Human BodySarah PavuNessuna valutazione finora
- Adeno VirusDocumento12 pagineAdeno VirusSarah PavuNessuna valutazione finora
- Cell Culture Reagents: Lithu - Radhakrishnan D3 BiotechDocumento10 pagineCell Culture Reagents: Lithu - Radhakrishnan D3 BiotechSarah PavuNessuna valutazione finora
- Chloroplast and PhotosynthesisDocumento19 pagineChloroplast and PhotosynthesisSarah Pavu50% (2)
- #PNEUMOCOCCUS#Documento11 pagine#PNEUMOCOCCUS#Sarah PavuNessuna valutazione finora
- Prokaryotic Cell-1Documento26 pagineProkaryotic Cell-1Sarah PavuNessuna valutazione finora
- Unit 16a G Protein Coupled ReceptorsDocumento6 pagineUnit 16a G Protein Coupled ReceptorsSarah PavuNessuna valutazione finora
- #Vibrio & Pseudomonas#Documento6 pagine#Vibrio & Pseudomonas#Sarah PavuNessuna valutazione finora
- # Enterobacteriaceaei#Documento7 pagine# Enterobacteriaceaei#Sarah PavuNessuna valutazione finora
- CMB NotesDocumento19 pagineCMB NotesSarah PavuNessuna valutazione finora
- Apoptosis Cell Bio Unit 4Documento17 pagineApoptosis Cell Bio Unit 4Sarah PavuNessuna valutazione finora
- Unit 15 Cell Junction DhanDocumento18 pagineUnit 15 Cell Junction DhanSarah PavuNessuna valutazione finora
- Unit 11 Cell AdesionDocumento15 pagineUnit 11 Cell AdesionSarah PavuNessuna valutazione finora
- Unit 10 Cell Cycle RegulationDocumento8 pagineUnit 10 Cell Cycle RegulationSarah PavuNessuna valutazione finora
- Unit 11 Cell AdesionDocumento15 pagineUnit 11 Cell AdesionSarah PavuNessuna valutazione finora
- CancerDocumento17 pagineCancerSarah PavuNessuna valutazione finora
- Pleural Fluid AspirationDocumento2 paginePleural Fluid AspirationThe Multilingual MedicNessuna valutazione finora
- Pathology MnemonicsDocumento18 paginePathology MnemonicsMamoorLatef100% (3)
- Anusol Ointment SPC SummaryDocumento3 pagineAnusol Ointment SPC SummarySanjay NavaleNessuna valutazione finora
- Cardiovascular Disease Nursing Diagnosis - Causes - FactsDocumento3 pagineCardiovascular Disease Nursing Diagnosis - Causes - Factsfeirri0% (1)
- Bioplasm-NLS Features Diagnostics SystemDocumento11 pagineBioplasm-NLS Features Diagnostics Systemdann kurokiNessuna valutazione finora
- Ataxia and Gait Disturbances: Presented by A. Hillier, D.O. EM Resident St. John West Shore HospitalDocumento21 pagineAtaxia and Gait Disturbances: Presented by A. Hillier, D.O. EM Resident St. John West Shore HospitalMaheswari DuraiNessuna valutazione finora
- General Surgery: Dr. S. Gallinge R Gord On Bud Uhan and Sam Minor, e D Itors Dana M Kay, Associate e D ItorDocumento56 pagineGeneral Surgery: Dr. S. Gallinge R Gord On Bud Uhan and Sam Minor, e D Itors Dana M Kay, Associate e D ItorKamran AfzalNessuna valutazione finora
- Clinical Protocols of NICUDocumento108 pagineClinical Protocols of NICUAmulya Ramakrishna100% (1)
- VestibulitisDocumento3 pagineVestibulitisDeniNessuna valutazione finora
- 13 - Radiology EmergencyDocumento60 pagine13 - Radiology EmergencykeluargacendanaNessuna valutazione finora
- Head InjuryDocumento50 pagineHead InjuryThiagarajah RaviNessuna valutazione finora
- Combined Pulmonary Fibrosis and Emphysema - Case Report and Literature ReviewDocumento6 pagineCombined Pulmonary Fibrosis and Emphysema - Case Report and Literature ReviewAMALIAHAKIMNessuna valutazione finora
- Tips by Masters of HomeopathyDocumento99 pagineTips by Masters of HomeopathyGeorge Montoya100% (3)
- Stephanie Russ Resume 1Documento2 pagineStephanie Russ Resume 1Ed C . HernandezNessuna valutazione finora
- Microbial Diseases of The Different Organ System SKINDocumento102 pagineMicrobial Diseases of The Different Organ System SKINBea Bianca CruzNessuna valutazione finora
- Respiratory Passmedicin 2022Documento1.020 pagineRespiratory Passmedicin 2022Faris Firas100% (1)
- RESUS 8904 Special CircsDocumento68 pagineRESUS 8904 Special CircsCroBranNessuna valutazione finora
- Otosclerosis: Causes, Symptoms and TreatmentDocumento25 pagineOtosclerosis: Causes, Symptoms and TreatmentHamid AliNessuna valutazione finora
- Oral Lichen Planus in Children ReportDocumento3 pagineOral Lichen Planus in Children ReportFebri YolandaNessuna valutazione finora
- Clinchers 100 Important PointsDocumento21 pagineClinchers 100 Important PointsNeha GoelNessuna valutazione finora
- Upper Urinary Tract. InfectionDocumento11 pagineUpper Urinary Tract. InfectionnadhifNessuna valutazione finora
- RheumatologygjjkjgvDocumento4 pagineRheumatologygjjkjgvShrayan DuttaNessuna valutazione finora
- Post Operative Management After TAPVC RepairDocumento36 paginePost Operative Management After TAPVC RepairsreedeviNessuna valutazione finora
- Prostate PamphletsDocumento2 pagineProstate PamphletsRich De GuzmanNessuna valutazione finora
- Bibliografía AngioVue Noviembre 2016Documento7 pagineBibliografía AngioVue Noviembre 2016Thomas Sanhueza VásquezNessuna valutazione finora
- Pathology and GeneticsDocumento11 paginePathology and Geneticssingireddi1revathi33% (3)
- AllianzDocumento27 pagineAllianzHariz SyahmiNessuna valutazione finora
- EDSnutritional SupplementsDocumento5 pagineEDSnutritional SupplementscaroNessuna valutazione finora
- MyxedemaDocumento3 pagineMyxedemaBobet ReñaNessuna valutazione finora
- MCQs LADocumento29 pagineMCQs LAPadmavathi C100% (1)