Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
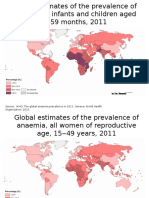
- Global Prevalence Anaemia 2011 MapsDocumento4 pagineGlobal Prevalence Anaemia 2011 MapsOktaviana Karyanti JuitaNessuna valutazione finora
- Classification of AnemiaDocumento8 pagineClassification of AnemiaFebrian ParuraNessuna valutazione finora
- Referat Current Treatment of OsteoarthritisDocumento72 pagineReferat Current Treatment of OsteoarthritisOktaviana Karyanti JuitaNessuna valutazione finora
- Morning ReportDocumento1 paginaMorning ReportOktaviana Karyanti JuitaNessuna valutazione finora
- Management of Ascites in CirrhosisDocumento38 pagineManagement of Ascites in CirrhosisOktaviana Karyanti JuitaNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Water On Mars PDFDocumento35 pagineWater On Mars PDFAlonso GarcíaNessuna valutazione finora
- AS 1 Pretest TOS S.Y. 2018-2019Documento2 pagineAS 1 Pretest TOS S.Y. 2018-2019Whilmark Tican MucaNessuna valutazione finora
- (Durt, - Christoph - Fuchs, - Thomas - Tewes, - Christian) Embodiment, Enaction, and Culture PDFDocumento451 pagine(Durt, - Christoph - Fuchs, - Thomas - Tewes, - Christian) Embodiment, Enaction, and Culture PDFnlf2205100% (3)
- Gothic Revival ArchitectureDocumento19 pagineGothic Revival ArchitectureAlexandra Maria NeaguNessuna valutazione finora
- NorthStar 5th Edition Reading-Writing SKILLS 3-4Documento265 pagineNorthStar 5th Edition Reading-Writing SKILLS 3-4Hassan JENZYNessuna valutazione finora
- Gigold PDFDocumento61 pagineGigold PDFSurender SinghNessuna valutazione finora
- The Integumentary System Development: Biene, Ellen Angelic Flores, Andrie BonDocumento29 pagineThe Integumentary System Development: Biene, Ellen Angelic Flores, Andrie BonMu Lok100% (3)
- DUN Bukit Lanjan CNY Sponsorship Form2Documento1 paginaDUN Bukit Lanjan CNY Sponsorship Form2alamsekitarselangorNessuna valutazione finora
- Biblehub Com Commentaries Matthew 3 17 HTMDocumento21 pagineBiblehub Com Commentaries Matthew 3 17 HTMSorin TrimbitasNessuna valutazione finora
- Navamsa Karma and GodDocumento9 pagineNavamsa Karma and GodVisti Larsen50% (2)
- Defending A Dogma: Between Grice, Strawson and Quine: Elvis ImafidonDocumento10 pagineDefending A Dogma: Between Grice, Strawson and Quine: Elvis ImafidonYang Wen-LiNessuna valutazione finora
- Amor Vs FlorentinoDocumento17 pagineAmor Vs FlorentinoJessica BernardoNessuna valutazione finora
- Week9 Phylum NemathelminthesDocumento26 pagineWeek9 Phylum NemathelminthesCzerinne Angela Justinne AlarillaNessuna valutazione finora
- Corporation Law Case Digests Philippines Merger and ConsolidationDocumento7 pagineCorporation Law Case Digests Philippines Merger and ConsolidationAlpha BetaNessuna valutazione finora
- Entity-Level Controls Fraud QuestionnaireDocumento8 pagineEntity-Level Controls Fraud QuestionnaireKirby C. LoberizaNessuna valutazione finora
- Reflection Paper-The Elephant Man PDFDocumento1 paginaReflection Paper-The Elephant Man PDFCarlosJohn02Nessuna valutazione finora
- Introduction To E-Business SystemsDocumento19 pagineIntroduction To E-Business SystemsArtur97% (79)
- Behaviour of Investors in Indian Equity Markets: Submitted byDocumento26 pagineBehaviour of Investors in Indian Equity Markets: Submitted byDibyanshu AmanNessuna valutazione finora
- RPT Form 2 2023Documento7 pagineRPT Form 2 2023NOREEN BINTI DOASA KPM-GuruNessuna valutazione finora
- Paradigm Shift in Teaching: The Plight of Teachers, Coping Mechanisms and Productivity in The New Normal As Basis For Psychosocial SupportDocumento5 pagineParadigm Shift in Teaching: The Plight of Teachers, Coping Mechanisms and Productivity in The New Normal As Basis For Psychosocial SupportPsychology and Education: A Multidisciplinary JournalNessuna valutazione finora
- Nin/Pmjay Id Name of The Vaccination Site Category Type District BlockDocumento2 pagineNin/Pmjay Id Name of The Vaccination Site Category Type District BlockNikunja PadhanNessuna valutazione finora
- PlayDocumento121 paginePlayellennelleNessuna valutazione finora
- Assignment Submission Form: Pgid Name of The MemberDocumento9 pagineAssignment Submission Form: Pgid Name of The MemberNamit GaurNessuna valutazione finora
- IUGRDocumento4 pagineIUGRMichael Spica RampangileiNessuna valutazione finora
- Oleracea Contain 13.2% Dry Matter, 15.7% Crude Protein, 5.4% Ether ExtractionDocumento47 pagineOleracea Contain 13.2% Dry Matter, 15.7% Crude Protein, 5.4% Ether ExtractionJakin Aia TapanganNessuna valutazione finora
- Bsed FilipinoDocumento18 pagineBsed FilipinoJ.PNessuna valutazione finora
- Binding of IsaacDocumento10 pagineBinding of IsaacBraz SouzaNessuna valutazione finora
- Debus Medical RenaissanceDocumento3 pagineDebus Medical RenaissanceMarijaNessuna valutazione finora
- Resume Testing6+ SaptagireswarDocumento5 pagineResume Testing6+ SaptagireswarSuresh RamasamyNessuna valutazione finora
- Marriage Practices Among The Gidda Oromo, Northern Wollega, EthiopiaDocumento2 pagineMarriage Practices Among The Gidda Oromo, Northern Wollega, Ethiopiajoseph mathewNessuna valutazione finora