Potrebbero piacerti anche
- Hip Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentDa EverandHip Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentNessuna valutazione finora
- Injuries Around The ShoulderDocumento81 pagineInjuries Around The ShoulderMisoNessuna valutazione finora
- DeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsDa EverandDeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNessuna valutazione finora
- Principles and Management of Acute Orthopaedic Trauma: Third EditionDa EverandPrinciples and Management of Acute Orthopaedic Trauma: Third EditionNessuna valutazione finora
- Upper Limb FractureDocumento15 pagineUpper Limb Fracturevivien kate perixNessuna valutazione finora
- Genu Recurvatum SyndromDocumento7 pagineGenu Recurvatum SyndromRoxana RascaNessuna valutazione finora
- Forearm Fractures PDFDocumento4 pagineForearm Fractures PDFNur Ashriawati BurhanNessuna valutazione finora
- Slipped Capital Femoral EpiphysisDocumento12 pagineSlipped Capital Femoral Epiphysisapi-26159412Nessuna valutazione finora
- Tendon Injuries of Hand: DR Saumya AgarwalDocumento101 pagineTendon Injuries of Hand: DR Saumya AgarwaltesfahuntekletilahunNessuna valutazione finora
- Handand Wrist ExammasterDocumento91 pagineHandand Wrist ExammasterjothiNessuna valutazione finora
- Hand PDFDocumento179 pagineHand PDFRadenSiwi Bagus HadhiningratNessuna valutazione finora
- Orthopedic: Dislocations of The Hip JointDocumento16 pagineOrthopedic: Dislocations of The Hip JointAnmarNessuna valutazione finora
- Physio4all... : Orthopaedics Assessment Sagar NaikDocumento9 paginePhysio4all... : Orthopaedics Assessment Sagar NaikRajeev Tiwari100% (2)
- Ankle Fractures - A Logical Approach To Their FixationDocumento48 pagineAnkle Fractures - A Logical Approach To Their FixationRoman MosneagaNessuna valutazione finora
- Tuberculosis of Hip JointDocumento25 pagineTuberculosis of Hip JointYousra ShaikhNessuna valutazione finora
- B 756 Vertebris GB III10Documento44 pagineB 756 Vertebris GB III10Lukasz Bartochowski100% (1)
- 3.5 MM LCP Anterolateral Distal de TibiaDocumento27 pagine3.5 MM LCP Anterolateral Distal de TibiaAlfredo AlfredoNessuna valutazione finora
- Hemiarthroplasty Hip - Apr20Documento10 pagineHemiarthroplasty Hip - Apr20Shalu OjhaNessuna valutazione finora
- Distal Femur (Sandeep Sir)Documento22 pagineDistal Femur (Sandeep Sir)Kirubakaran Saraswathy PattabiramanNessuna valutazione finora
- Examination of Hand & Common Hand InjuriesDocumento165 pagineExamination of Hand & Common Hand InjuriesPriya GK100% (1)
- Low Back Pain: Rezki Amalia NurshalDocumento74 pagineLow Back Pain: Rezki Amalia NurshalRezki Amalia NurshalNessuna valutazione finora
- Evaluation of The Hand!Documento84 pagineEvaluation of The Hand!Ahmad A. Fannoon100% (1)
- Biomech of Hip JointDocumento68 pagineBiomech of Hip JointkashifNessuna valutazione finora
- Wrist Anatomy and Surgical ApproachesDocumento19 pagineWrist Anatomy and Surgical ApproacheswilhelmNessuna valutazione finora
- Acl Injury Surgery - Orthoinfo - AaosDocumento15 pagineAcl Injury Surgery - Orthoinfo - Aaosapi-228773845Nessuna valutazione finora
- Acute Management Pelvic RingDocumento91 pagineAcute Management Pelvic RingClever ImaniaNessuna valutazione finora
- Tendon InjuriesDocumento48 pagineTendon InjuriesdiasNessuna valutazione finora
- Bio Mechanics of The Wrist and HandDocumento50 pagineBio Mechanics of The Wrist and HandOnwaree Ing100% (6)
- Trauma & Orthopaedic SurgeryDocumento120 pagineTrauma & Orthopaedic SurgeryOstazNessuna valutazione finora
- Scapular DyskinesisDocumento24 pagineScapular DyskinesisbarbaraNessuna valutazione finora
- Surgical ApproachDocumento124 pagineSurgical ApproachHendra AjahNessuna valutazione finora
- Biomechanics of SpineDocumento49 pagineBiomechanics of SpineDheerajJonnalagaddaNessuna valutazione finora
- IvdpDocumento89 pagineIvdpFelix SabuNessuna valutazione finora
- Degenerative Diseases of SpineDocumento115 pagineDegenerative Diseases of SpineCodillia CheongNessuna valutazione finora
- Low Back Exam PDFDocumento2 pagineLow Back Exam PDFDeeea1991Nessuna valutazione finora
- CTEVDocumento61 pagineCTEVSylvia LoongNessuna valutazione finora
- Genu VarumDocumento12 pagineGenu VarumPutri DwiridalNessuna valutazione finora
- Club Foot-Dr J SahooDocumento9 pagineClub Foot-Dr J SahooSheel Gupta100% (1)
- Ortho Special TestsDocumento254 pagineOrtho Special TestsLaura LauraaNessuna valutazione finora
- Orthopedics Ebook Notes PDFDocumento42 pagineOrthopedics Ebook Notes PDFSofia Love100% (1)
- Anatomy of The SpineDocumento83 pagineAnatomy of The SpineUkhti Nur Zannah83% (6)
- Office Orthopaedics: Ramirez, Bryan Paul GDocumento57 pagineOffice Orthopaedics: Ramirez, Bryan Paul GBryan Paul RamirezNessuna valutazione finora
- Ankle and Foot Examination PDFDocumento16 pagineAnkle and Foot Examination PDFainizatiNessuna valutazione finora
- Physical Examination of The Shoulder FinalDocumento28 paginePhysical Examination of The Shoulder FinalAndinNessuna valutazione finora
- Upper Limb OrthosisDocumento83 pagineUpper Limb OrthosisAwaisNessuna valutazione finora
- Cervical Stenosis 2006Documento16 pagineCervical Stenosis 2006kppsadiNessuna valutazione finora
- Cervical Spine Stomatognatic System and CraniofacialDocumento40 pagineCervical Spine Stomatognatic System and CraniofacialDenise MathreNessuna valutazione finora
- Lower Limb Fracture..MeDocumento142 pagineLower Limb Fracture..MeWorku KifleNessuna valutazione finora
- Orthopaedic AnatomyDocumento1 paginaOrthopaedic Anatomyintan rosliNessuna valutazione finora
- Cervical SpondylosisDocumento9 pagineCervical SpondylosisNurHidayah Borhanudin100% (1)
- Management of The Floating Knee.Documento8 pagineManagement of The Floating Knee.barbara liuva chia policarpoNessuna valutazione finora
- Ankle Arthrodesis - Screw FixationDocumento26 pagineAnkle Arthrodesis - Screw FixationChristopher HoodNessuna valutazione finora
- Traction in OrthopaedicDocumento32 pagineTraction in OrthopaedicFarry Doank100% (1)
- Wrist Anatomy: Bones Quiz - What Bones Comprise The Wrist? Joints Quiz - What Joints Comprise The Wrist?Documento63 pagineWrist Anatomy: Bones Quiz - What Bones Comprise The Wrist? Joints Quiz - What Joints Comprise The Wrist?Mnn SaabNessuna valutazione finora
- Humerus FractureDocumento18 pagineHumerus FractureHęñøķ BęŕhãñęNessuna valutazione finora
- Biomechanics Ankle PresentationDocumento10 pagineBiomechanics Ankle Presentationx.cortez100% (1)
- Proximal Femoral NewDocumento34 pagineProximal Femoral NewHimanshu HemantNessuna valutazione finora
- Anatomy of HandDocumento54 pagineAnatomy of Handromaisa akhtar100% (1)
- Lower Extremity Orthosis: Noel R. San Antonio, PTRP MSCPDDocumento27 pagineLower Extremity Orthosis: Noel R. San Antonio, PTRP MSCPDLeo LopezNessuna valutazione finora
- Coronary Arterial Disease: S Chapter 60 1657Documento26 pagineCoronary Arterial Disease: S Chapter 60 1657Staen KisNessuna valutazione finora
- Congenital Heart DefectsDocumento73 pagineCongenital Heart DefectsStaen KisNessuna valutazione finora
- Congenital Heart DefectsDocumento73 pagineCongenital Heart DefectsStaen KisNessuna valutazione finora
- Caesarean SectionDocumento48 pagineCaesarean SectionStaen KisNessuna valutazione finora
- Color Atlas of Surgical Approaches To The Bones and Joints of The Dog and CatDocumento245 pagineColor Atlas of Surgical Approaches To The Bones and Joints of The Dog and CatScott Rose100% (8)
- Unit 5 Anatomy and Physiology in Health and Social CareDocumento53 pagineUnit 5 Anatomy and Physiology in Health and Social Caremurdatwotimes90% (31)
- Class 9 Project No. 2 2021 2022Documento34 pagineClass 9 Project No. 2 2021 2022priyanshuprasad27150Nessuna valutazione finora
- Microsoft Word - The Skeletal SystemDocumento24 pagineMicrosoft Word - The Skeletal SystemNino Alania0% (2)
- 5-Locomotion and Movement PDFDocumento4 pagine5-Locomotion and Movement PDFPraveen KumarNessuna valutazione finora
- Movement Analysis FinalDocumento18 pagineMovement Analysis FinalAaron NicolNessuna valutazione finora
- Radiographic Positioning: (Reinforcement)Documento646 pagineRadiographic Positioning: (Reinforcement)BeverlyNessuna valutazione finora
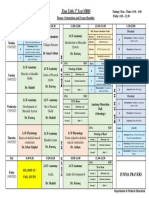
- Timetable 1st Year MBBS MSK Module Week 2Documento1 paginaTimetable 1st Year MBBS MSK Module Week 2UZAIR KHANNessuna valutazione finora
- Physical Examination of The Shoulder FinalDocumento28 paginePhysical Examination of The Shoulder FinalAndinNessuna valutazione finora
- Skeletal SystemDocumento17 pagineSkeletal SystemRachell AvecillaNessuna valutazione finora
- Kebo120 PDFDocumento13 pagineKebo120 PDFRitesh SalunkeNessuna valutazione finora
- Chapter 3 Musculoskeletal Systems Part 2Documento106 pagineChapter 3 Musculoskeletal Systems Part 2kamalab04Nessuna valutazione finora
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocumento7 pagineSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNessuna valutazione finora
- Javelin Throw Bio MechanicsDocumento14 pagineJavelin Throw Bio MechanicsSandipan DasSarma100% (2)
- 5 Chapter AnaphyDocumento8 pagine5 Chapter Anaphyjeanbecera19Nessuna valutazione finora
- Jens Waschke (Editor), Tobias M. Böckers (Editor), Friedrich Paulsen (Editor) - Sobotta Anatomy Textbook - With Latin Nomenclature-Educa Books (2018) PDFDocumento843 pagineJens Waschke (Editor), Tobias M. Böckers (Editor), Friedrich Paulsen (Editor) - Sobotta Anatomy Textbook - With Latin Nomenclature-Educa Books (2018) PDFЙоана Георгиева100% (2)
- PE 1 Midterm Exam 2022Documento3 paginePE 1 Midterm Exam 202212 S1 Delos Santos Doreen Claire M.Nessuna valutazione finora
- Appendicular SkeletonDocumento23 pagineAppendicular SkeletonFachriza Effendi100% (1)
- OnBaseU Pitching Manual NotesDocumento5 pagineOnBaseU Pitching Manual Noteslw98Nessuna valutazione finora
- Comparison of Three Stretches For The Pectoralis Minor Muscle PDFDocumento7 pagineComparison of Three Stretches For The Pectoralis Minor Muscle PDFsebafigueroa94Nessuna valutazione finora
- PyomyositisDocumento17 paginePyomyositisiluvmypoopoo22100% (1)
- Test Bank For Anatomy Physiology 2nd Edition Martini NashDocumento41 pagineTest Bank For Anatomy Physiology 2nd Edition Martini Nashjavierdoyleafkqexcgzj100% (38)
- '05 Sullivan C.Documento37 pagine'05 Sullivan C.Geo Navarro100% (1)
- BD Chaurasiya Human Anatomy For Dental StudentsDocumento714 pagineBD Chaurasiya Human Anatomy For Dental StudentsBhumika Sharma100% (14)
- Appendicular Worksheet With Answers ch.11Documento7 pagineAppendicular Worksheet With Answers ch.11Alejandra ReynaNessuna valutazione finora
- Form 5 Biology Perfect Score Paper 1 Topical Exercise E ModuleDocumento156 pagineForm 5 Biology Perfect Score Paper 1 Topical Exercise E Modulewickedbiology10188% (8)
- Locomotion and MovementDocumento9 pagineLocomotion and MovementRamanna ChowdaryNessuna valutazione finora
- LAFD - Wellness and Fitness Exercise Manual (2004) 63p R20090725DDocumento63 pagineLAFD - Wellness and Fitness Exercise Manual (2004) 63p R20090725DfilzovocNessuna valutazione finora
- Moore's Clinically Oriented Anatomy 6th EdDocumento4 pagineMoore's Clinically Oriented Anatomy 6th EdJohna Pauline Mandac67% (6)
- Clinical Anatomy of The Upper Limb: Kara Mudd, MSPAS, PA-CDocumento51 pagineClinical Anatomy of The Upper Limb: Kara Mudd, MSPAS, PA-CMariumNessuna valutazione finora