Potrebbero piacerti anche
- Fibroids Miracle Cure: The Ultimate Fibroids Diet To Heal NaturallyDa EverandFibroids Miracle Cure: The Ultimate Fibroids Diet To Heal NaturallyValutazione: 3.5 su 5 stelle3.5/5 (7)
- Theory of Myoma Uteri: Gede Nanda Surya WijayaDocumento32 pagineTheory of Myoma Uteri: Gede Nanda Surya WijayaNandaSuryaWijayaNessuna valutazione finora
- 9 MyomaDocumento36 pagine9 MyomaDawit g/kidanNessuna valutazione finora
- Fibroid Uterus 2019Documento60 pagineFibroid Uterus 2019Mahmoud Abu Al AmrainNessuna valutazione finora
- Benign Diseases of Cervix, Uterus & OvaryDocumento58 pagineBenign Diseases of Cervix, Uterus & OvaryFaheem HassanNessuna valutazione finora
- Path Pathology of The Uterus Part 1 2020-2021Documento7 paginePath Pathology of The Uterus Part 1 2020-2021JohnNessuna valutazione finora
- Uterine FibroidsDocumento25 pagineUterine FibroidsMarie Eulie PatinoNessuna valutazione finora
- Uterine Leiyomyoma and PolypsDocumento68 pagineUterine Leiyomyoma and PolypsKilp MosesNessuna valutazione finora
- Uterine FibroidsDocumento25 pagineUterine FibroidssyifasfNessuna valutazione finora
- Benignlesionshanisah 161129150208Documento71 pagineBenignlesionshanisah 161129150208Mohammad Saadullah Khan KakarNessuna valutazione finora
- Myoma EndometrialDocumento26 pagineMyoma EndometrialYulia PratiwiNessuna valutazione finora
- Endometriosis O&g PresentationDocumento31 pagineEndometriosis O&g PresentationChauthiran Agamudaiyar100% (1)
- Uterine Myoma, Sept, 2021Documento63 pagineUterine Myoma, Sept, 2021Kerod AbebeNessuna valutazione finora
- Ovarian Cyst and TumorDocumento37 pagineOvarian Cyst and TumorDr Mayusha SawantNessuna valutazione finora
- Adult WomenDocumento57 pagineAdult Womenmarron35patricioNessuna valutazione finora
- Uterine Fibroid-IzzatDocumento20 pagineUterine Fibroid-IzzatcopperNessuna valutazione finora
- Benign ConditionsDocumento40 pagineBenign ConditionsnoreenfatimamaanNessuna valutazione finora
- Chapter 4Documento9 pagineChapter 4Lennie LennieNessuna valutazione finora
- 1.TUM Benigne UterinaDocumento47 pagine1.TUM Benigne UterinaPavel BerlinschiNessuna valutazione finora
- Lecture - Eight - Care - of - Women - With - EndometriosisDocumento22 pagineLecture - Eight - Care - of - Women - With - EndometriosisOmar SanyangNessuna valutazione finora
- Uterine Fibroids Are NoncancerousDocumento3 pagineUterine Fibroids Are NoncancerousNeha BhasinNessuna valutazione finora
- Fibroids: DR F HoveDocumento18 pagineFibroids: DR F HoveKelvin MaikanaNessuna valutazione finora
- Myoma Treatment Options MR Guided Focused Ultrasound (Mrgfus)Documento3 pagineMyoma Treatment Options MR Guided Focused Ultrasound (Mrgfus)Marvi Hollanda SalandananNessuna valutazione finora
- EndometriosisDocumento50 pagineEndometriosisHannah Eloise MagsinoNessuna valutazione finora
- Effects of Aging in Endocrine SystemDocumento5 pagineEffects of Aging in Endocrine Systemapi-3718174Nessuna valutazione finora
- Liomyoma (Fibroid) : DR Henan DH Skheel 2016 5 Year Directed LectureDocumento11 pagineLiomyoma (Fibroid) : DR Henan DH Skheel 2016 5 Year Directed LectureAnonymous UHnQSkxLBDNessuna valutazione finora
- Fibroid Uterus NewDocumento98 pagineFibroid Uterus NewBi PinNessuna valutazione finora
- Breast Tumors.Documento23 pagineBreast Tumors.jabarinjamalsajaNessuna valutazione finora
- Breast CancerDocumento69 pagineBreast CancerRayanNessuna valutazione finora
- Also Called Uterine Leiomyoma, Myoma, Myomata Uteri, FibromyomaDocumento25 pagineAlso Called Uterine Leiomyoma, Myoma, Myomata Uteri, Fibromyomashygirl72Nessuna valutazione finora
- Benign Tumors of Female Genital OrgansDocumento37 pagineBenign Tumors of Female Genital Organssimi yNessuna valutazione finora
- By: Mimi Suhaini BT Sudin 030.08.308 Kepaniteraan Ilmu Kandungan Dan Kebidanan RSAL Fakultas Kedokteran TrisaktiDocumento11 pagineBy: Mimi Suhaini BT Sudin 030.08.308 Kepaniteraan Ilmu Kandungan Dan Kebidanan RSAL Fakultas Kedokteran TrisaktiMimi Suhaini SudinNessuna valutazione finora
- Uterine FibroidsDocumento47 pagineUterine FibroidsMoh Aldhy HusaintNessuna valutazione finora
- 4.. ReproDocumento61 pagine4.. Reprosabin luitelNessuna valutazione finora
- Uterine PolypDocumento27 pagineUterine PolypThanujaa UvarajNessuna valutazione finora
- Uterine FibroidsDocumento46 pagineUterine FibroidsRavindranatha AnNessuna valutazione finora
- Abnormal Uterine BleedingDocumento28 pagineAbnormal Uterine BleedingHuzaifaNessuna valutazione finora
- Uterine FibroidsDocumento46 pagineUterine FibroidsErwynsonsaut SimanjuntakNessuna valutazione finora
- Dysfunctional Uterine Bleeding Lecture DR Gem AshbyDocumento45 pagineDysfunctional Uterine Bleeding Lecture DR Gem AshbyPandawa ObgynNessuna valutazione finora
- Benign Breast DisordersDocumento30 pagineBenign Breast DisordersShams Nadeem AlamNessuna valutazione finora
- Endometriosis & AdenomyosisDocumento54 pagineEndometriosis & AdenomyosisKapil StaleyNessuna valutazione finora
- Benign Disorders and Diseases of The BreastDocumento44 pagineBenign Disorders and Diseases of The BreastRoy Acosta GumbanNessuna valutazione finora
- ENDOMETRIOSISDocumento33 pagineENDOMETRIOSISpriyanka bhowmikNessuna valutazione finora
- ENDOMETRIOSISDocumento29 pagineENDOMETRIOSISMaria ClaraNessuna valutazione finora
- Benign and Malignant Tumor of UterusDocumento138 pagineBenign and Malignant Tumor of UterusMuhammad HaziqNessuna valutazione finora
- Myoma Uteri/Fibroids/ Leiomyomata: Symptoms of Uterine Myoma May IncludeDocumento3 pagineMyoma Uteri/Fibroids/ Leiomyomata: Symptoms of Uterine Myoma May IncludeDiane MargretNessuna valutazione finora
- Myoma Uteri: Pregnancy PubertyDocumento9 pagineMyoma Uteri: Pregnancy PubertyJaja RamosNessuna valutazione finora
- Different Pathologies of The UterusDocumento74 pagineDifferent Pathologies of The UterusAmal100% (1)
- Uterine Fibroids: By: DR Dolapo AduDocumento35 pagineUterine Fibroids: By: DR Dolapo AduAdu DolapoNessuna valutazione finora
- Female Reproductive - 3, Dub, Uterus Lesions, Turner SyndromeDocumento34 pagineFemale Reproductive - 3, Dub, Uterus Lesions, Turner Syndromeindu mathiNessuna valutazione finora
- Uterine LeiomyomaDocumento57 pagineUterine LeiomyomaRomy Mansour100% (2)
- Benign Dis of The UterusDocumento22 pagineBenign Dis of The UterusAsraa RashedNessuna valutazione finora
- Fibroids PresentationDocumento6 pagineFibroids Presentationapi-237061134Nessuna valutazione finora
- Benign Neoplasms of The Genital 2Documento22 pagineBenign Neoplasms of The Genital 2ugonna nwokeNessuna valutazione finora
- Care of Patients With Cancer of The Cervix and UterusDocumento13 pagineCare of Patients With Cancer of The Cervix and UterusJumar ValdezNessuna valutazione finora
- General Objective:: JERIEL Pregnancy-Related BleedingDocumento6 pagineGeneral Objective:: JERIEL Pregnancy-Related BleedingJim Christian EllaserNessuna valutazione finora
- OB-GYN 101: Uterine LeiomyomaDocumento3 pagineOB-GYN 101: Uterine Leiomyomamadmax500Nessuna valutazione finora
- Benign Breast Disease111Documento55 pagineBenign Breast Disease111Gowtham GanesanNessuna valutazione finora
- Benign Neoplasm of OvaryDocumento60 pagineBenign Neoplasm of OvaryMimie SabrinaNessuna valutazione finora
- Abnormal Uterine Bleeding FinalDocumento133 pagineAbnormal Uterine Bleeding FinalMLV AbayNessuna valutazione finora
- Kul Sem 4 Heat Stroke N Fever UHT 2016Documento63 pagineKul Sem 4 Heat Stroke N Fever UHT 2016NandaSuryaWijayaNessuna valutazione finora
- Bso CairDocumento37 pagineBso CairNanda ValeriadiNessuna valutazione finora
- IKM - TB Di Puskesmas - Wienta - April 2018 PDFDocumento40 pagineIKM - TB Di Puskesmas - Wienta - April 2018 PDFNandaSuryaWijayaNessuna valutazione finora
- Rational U: Se of DrugsDocumento27 pagineRational U: Se of DrugsNandaSuryaWijayaNessuna valutazione finora
- Prospective Study of Alcohol Consumption and MetabolicDocumento9 pagineProspective Study of Alcohol Consumption and MetabolicNandaSuryaWijayaNessuna valutazione finora
- Kul Sem 4 Heat Stroke N Fever UHT 2016Documento63 pagineKul Sem 4 Heat Stroke N Fever UHT 2016NandaSuryaWijayaNessuna valutazione finora
- AbstractDocumento1 paginaAbstractNandaSuryaWijayaNessuna valutazione finora
- Alcohol Consumption and The PrevalenceDocumento6 pagineAlcohol Consumption and The PrevalenceNandaSuryaWijayaNessuna valutazione finora
- Effect of Ethanol On Metabolic SyndromeDocumento5 pagineEffect of Ethanol On Metabolic SyndromeNandaSuryaWijayaNessuna valutazione finora
- ESPEN Guidelines On Parenteral NutritionDocumento9 pagineESPEN Guidelines On Parenteral NutritionNandaSuryaWijayaNessuna valutazione finora
- What Is Metabolic Syndrome?: HeartDocumento2 pagineWhat Is Metabolic Syndrome?: HeartNandaSuryaWijayaNessuna valutazione finora
- Task SurgeryDocumento1 paginaTask SurgeryNandaSuryaWijayaNessuna valutazione finora
- Histo 61Documento3 pagineHisto 61NandaSuryaWijayaNessuna valutazione finora
- AbstractDocumento1 paginaAbstractNandaSuryaWijayaNessuna valutazione finora
- Prosedur Transfusi SecureDocumento65 pagineProsedur Transfusi SecureNandaSuryaWijayaNessuna valutazione finora
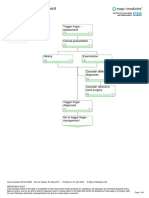
- Trigger Finger PostopDocumento2 pagineTrigger Finger PostopNandaSuryaWijayaNessuna valutazione finora
- Nasronudin., 2007. Penyakit Infeksi Di Indonesia Solusi Kini Dan Mendatang. Airlangga University Press, Surabaya. 4Documento1 paginaNasronudin., 2007. Penyakit Infeksi Di Indonesia Solusi Kini Dan Mendatang. Airlangga University Press, Surabaya. 4NandaSuryaWijayaNessuna valutazione finora
- TriggerFinger PDFDocumento1 paginaTriggerFinger PDFNandaSuryaWijayaNessuna valutazione finora
- Trigger Finger 21-01-10Documento6 pagineTrigger Finger 21-01-10NandaSuryaWijayaNessuna valutazione finora
- Trigger Finger 2Documento3 pagineTrigger Finger 2NandaSuryaWijayaNessuna valutazione finora
- Dapus MiomaDocumento2 pagineDapus MiomaNandaSuryaWijayaNessuna valutazione finora
- Ranitidine Is An Antagonist of Histamine at Gastric H2Documento2 pagineRanitidine Is An Antagonist of Histamine at Gastric H2NandaSuryaWijayaNessuna valutazione finora
- Myoma NewwwDocumento46 pagineMyoma NewwwNandaSuryaWijayaNessuna valutazione finora
- Daftar Pustaka BPHDocumento1 paginaDaftar Pustaka BPHNandaSuryaWijayaNessuna valutazione finora
- Table of ContentsDocumento3 pagineTable of ContentsNandaSuryaWijayaNessuna valutazione finora
- CAKUTDocumento50 pagineCAKUTsantosh subediNessuna valutazione finora
- Consumer PresentationDocumento30 pagineConsumer PresentationShafiqur Rahman KhanNessuna valutazione finora
- Balkhu Squatter SettlementDocumento10 pagineBalkhu Squatter SettlementShramina ShresthaNessuna valutazione finora
- BTL Marketing CompanyDocumento30 pagineBTL Marketing Companypradip_kumarNessuna valutazione finora
- Travel OrderDocumento2 pagineTravel OrderStephen EstalNessuna valutazione finora
- Software Requirements SpecificationDocumento9 pagineSoftware Requirements SpecificationSu-kEm Tech LabNessuna valutazione finora
- VHP Series Five P9394Gsi S5: With Esm2 and Empact Emission Control SystemDocumento2 pagineVHP Series Five P9394Gsi S5: With Esm2 and Empact Emission Control SystemGabrielito PachacamaNessuna valutazione finora
- 2062 TSSR Site Sharing - Rev02Documento44 pagine2062 TSSR Site Sharing - Rev02Rio DefragNessuna valutazione finora
- AXIOM75 50 25 1B - Rev.6 10.000MHzDocumento4 pagineAXIOM75 50 25 1B - Rev.6 10.000MHzTürkay PektürkNessuna valutazione finora
- Unknown 31Documento40 pagineUnknown 31Tina TinaNessuna valutazione finora
- Plant Gardening AerationDocumento4 paginePlant Gardening Aerationut.testbox7243Nessuna valutazione finora
- Updated PDPDocumento540 pagineUpdated PDPnikulaaaasNessuna valutazione finora
- What Are The Challenges and Opportunities of ResearchingDocumento5 pagineWhat Are The Challenges and Opportunities of ResearchingmelkyNessuna valutazione finora
- LOMA FLMI CoursesDocumento4 pagineLOMA FLMI CoursesCeleste Joy C. LinsanganNessuna valutazione finora
- E-Cat35xt014 Xtro PhantomsDocumento32 pagineE-Cat35xt014 Xtro PhantomsKari Wilfong100% (5)
- Inclusions in Gross IncomeDocumento2 pagineInclusions in Gross Incomeloonie tunesNessuna valutazione finora
- Iot Practical 1Documento15 pagineIot Practical 1A26Harsh KalokheNessuna valutazione finora
- KVM Architecture OverviewDocumento15 pagineKVM Architecture Overviewdattbbk1Nessuna valutazione finora
- Defence QuestionnaireDocumento2 pagineDefence QuestionnaireSumitt SinghNessuna valutazione finora
- A Study On Awareness of Mutual Funds and Perception of Investors 2Documento89 pagineA Study On Awareness of Mutual Funds and Perception of Investors 2Yashaswini BangeraNessuna valutazione finora
- Genstat Release 10.3de (Pc/Windows 7) 28 May 2012 06:35:59Documento6 pagineGenstat Release 10.3de (Pc/Windows 7) 28 May 2012 06:35:59Anna Nur HidayatiNessuna valutazione finora
- Generalised Ultimate Loads For Pile GroupsDocumento22 pagineGeneralised Ultimate Loads For Pile GroupsValerioNessuna valutazione finora
- Mechanical Power FormulaDocumento9 pagineMechanical Power FormulaEzeBorjesNessuna valutazione finora
- RRC & RabDocumento14 pagineRRC & RabSyed Waqas AhmedNessuna valutazione finora
- Material List Summary-WaptechDocumento5 pagineMaterial List Summary-WaptechMarko AnticNessuna valutazione finora
- Zoomlion Gulf FZE Introduction: 1.1 ME Service Support 1.2 Construction CasesDocumento13 pagineZoomlion Gulf FZE Introduction: 1.1 ME Service Support 1.2 Construction CasesArk TradingNessuna valutazione finora
- Homework 1 Tarea 1Documento11 pagineHomework 1 Tarea 1Anette Wendy Quipo Kancha100% (1)
- Opening The Third EyeDocumento13 pagineOpening The Third EyekakamacgregorNessuna valutazione finora
- Ingredients EnsaymadaDocumento3 pagineIngredients Ensaymadajessie OcsNessuna valutazione finora
- Aggregate Production PlanningDocumento5 pagineAggregate Production PlanningSarbani SahuNessuna valutazione finora