Potrebbero piacerti anche
- RA & SLE Kuliah Blok 2014 EditDocumento75 pagineRA & SLE Kuliah Blok 2014 EditAdi ParamarthaNessuna valutazione finora
- Medical Surgical Nursing: Musculoskeletal Alterations: Section 1 InfectionsDocumento46 pagineMedical Surgical Nursing: Musculoskeletal Alterations: Section 1 InfectionsmyatchNessuna valutazione finora
- Rheumatoid ArthritisDocumento62 pagineRheumatoid ArthritisChuah Wei HongNessuna valutazione finora
- Lo PlenoDocumento100 pagineLo PlenoBilqis ElfariantiNessuna valutazione finora
- Classification of Disorders of Musculoskeletal System (MSK) : Presented By: Siti Sarah Maha Dewi Bong Jen NeeDocumento69 pagineClassification of Disorders of Musculoskeletal System (MSK) : Presented By: Siti Sarah Maha Dewi Bong Jen NeeBONG AIKCHINGNessuna valutazione finora
- Rheumatology Year 4Documento90 pagineRheumatology Year 4Abdalla SamatarNessuna valutazione finora
- 3RD OrvDocumento18 pagine3RD OrvJulienne HernandezNessuna valutazione finora
- Joint Pain - ClassDocumento88 pagineJoint Pain - ClassPrecious ChaiNessuna valutazione finora
- Donna-Marie Mcmahon, Do, Faap Kathleen M. Vazzana, Do, MsDocumento13 pagineDonna-Marie Mcmahon, Do, Faap Kathleen M. Vazzana, Do, MsMuhammad GassanNessuna valutazione finora
- Approach To Arthritis PDFDocumento54 pagineApproach To Arthritis PDFanahitshoNessuna valutazione finora
- Sle-Pdui 12 Maret 2010aDocumento59 pagineSle-Pdui 12 Maret 2010aYudha SavestilaNessuna valutazione finora
- Juvenile Idiopathic Arthritis JIA or JRA: What's in A Name?Documento63 pagineJuvenile Idiopathic Arthritis JIA or JRA: What's in A Name?Rajesh BalakrishnanNessuna valutazione finora
- Rheumatoid ArthritisDocumento29 pagineRheumatoid ArthritisTamim IshtiaqueNessuna valutazione finora
- OSTEOARTHRITIS AND RHEUMATOID DISEASESDocumento80 pagineOSTEOARTHRITIS AND RHEUMATOID DISEASESfeby faradillaNessuna valutazione finora
- SLE & RA Guide: Diagnosis, Symptoms & TreatmentDocumento65 pagineSLE & RA Guide: Diagnosis, Symptoms & TreatmentJendrianiNessuna valutazione finora
- Rheumatoid ArthritisDocumento66 pagineRheumatoid ArthritisSaeda AhmedNessuna valutazione finora
- Medicine Seminar: Sakshi Malik 379 Shalini Singh 384 Sunanda Verma 394Documento53 pagineMedicine Seminar: Sakshi Malik 379 Shalini Singh 384 Sunanda Verma 394966342Nessuna valutazione finora
- Autoimmune Disease in ChildrenDocumento41 pagineAutoimmune Disease in ChildrenAulya ArchuletaNessuna valutazione finora
- Disorder of Musculo.system. Leatest PptxDocumento178 pagineDisorder of Musculo.system. Leatest PptxCheru TecheNessuna valutazione finora
- Rheumatology Notes From DR Osama LecturesDocumento76 pagineRheumatology Notes From DR Osama LecturesMohamed ElAyadiNessuna valutazione finora
- Ra FinaleDocumento80 pagineRa FinaleJoanaNessuna valutazione finora
- Rheum PPT 2018Documento58 pagineRheum PPT 2018Verónica Duménez JofréNessuna valutazione finora
- 2016 Resident's Pediatric Rheumatology GuideDocumento108 pagine2016 Resident's Pediatric Rheumatology GuideReba John100% (1)
- Musculoskeletal Autoimmune Disorders: RA, SLE, SclerodermaDocumento51 pagineMusculoskeletal Autoimmune Disorders: RA, SLE, SclerodermaSaya MenangNessuna valutazione finora
- باطنة تمريض rheumatologyDocumento6 pagineباطنة تمريض rheumatologyAbdullmlik AlfurasNessuna valutazione finora
- Case Report Rheumatoid ArthritisDocumento29 pagineCase Report Rheumatoid ArthritisEmmy Safitri Abbas0% (1)
- Chapter 54 Assessment and Management of Patients With Rheumatic DisordersDocumento19 pagineChapter 54 Assessment and Management of Patients With Rheumatic DisordersMaryrose GestosoNessuna valutazione finora
- ARTHRITIS-by Ayesigwa GeraldDocumento38 pagineARTHRITIS-by Ayesigwa GeraldAyesigwa Gerald96Nessuna valutazione finora
- Pathophysiology-Progressive Deterioration and Loss ofDocumento6 paginePathophysiology-Progressive Deterioration and Loss ofUSC Upstate Nursing CoachesNessuna valutazione finora
- Faculty of MedicineDocumento28 pagineFaculty of MedicineRana AtefNessuna valutazione finora
- Juvenile Rheumatoid Arthritis: Jeffrey A. LuceroDocumento10 pagineJuvenile Rheumatoid Arthritis: Jeffrey A. LucerojamilliumNessuna valutazione finora
- Reiter's SyndromeDocumento17 pagineReiter's SyndromeSyed Khidir Al-AminNessuna valutazione finora
- Juvenile Idiopathic ArthritisDocumento52 pagineJuvenile Idiopathic ArthritishasanajNessuna valutazione finora
- Speciality: General Medicine Case: Nephrotic Syndrome HistoryDocumento49 pagineSpeciality: General Medicine Case: Nephrotic Syndrome Historydrtpk100% (2)
- Juvenile Rheumatoid ArthritisDocumento30 pagineJuvenile Rheumatoid ArthritisAnonymous dFSZ2k2IUNessuna valutazione finora
- Reumato and EndocrineDocumento106 pagineReumato and Endocrinehasanatiya41Nessuna valutazione finora
- Diff DGX: SLE, Bursitis or Tendinitis, Polymyositis, Myofascial PainDocumento5 pagineDiff DGX: SLE, Bursitis or Tendinitis, Polymyositis, Myofascial PainCarissa CorraroNessuna valutazione finora
- Rheumatology MRCP1Documento186 pagineRheumatology MRCP1Raouf Ra'fat Soliman100% (3)
- Arthritides 5th Year-UNZA LectureDocumento76 pagineArthritides 5th Year-UNZA LectureMohammed AadeelNessuna valutazione finora
- Final Rheumatoid ArthritisDocumento27 pagineFinal Rheumatoid ArthritisAmmarNessuna valutazione finora
- Case Study Rheumatoid ArthritisDocumento16 pagineCase Study Rheumatoid ArthritisJessy Mallo100% (2)
- Tutor Susah Banget FinalDocumento25 pagineTutor Susah Banget FinalSani muzakirNessuna valutazione finora
- Juvenile RaDocumento27 pagineJuvenile RaEdwardNessuna valutazione finora
- Rheumatoid Arthritis (RA)Documento16 pagineRheumatoid Arthritis (RA)AL-ashai MohammedNessuna valutazione finora
- Musculoskeletal: Autoimmune Inflammatory Metabolic Infectious DisordersDocumento51 pagineMusculoskeletal: Autoimmune Inflammatory Metabolic Infectious DisordersHarshoi KrishannaNessuna valutazione finora
- ABIM Logy Review 2010Documento111 pagineABIM Logy Review 2010grahamabraNessuna valutazione finora
- Juvenile Idiopathic ArthritisDocumento52 pagineJuvenile Idiopathic ArthritispramitaNessuna valutazione finora
- Juvenile Idiopathic ArthritisDocumento4 pagineJuvenile Idiopathic ArthritisAmmarNessuna valutazione finora
- Systemic LupusDocumento25 pagineSystemic LupusRana AtefNessuna valutazione finora
- Approach Patient With ArthritisDocumento45 pagineApproach Patient With ArthritisAli TawbeNessuna valutazione finora
- Ra Sle MSDocumento60 pagineRa Sle MSDionisius KevinNessuna valutazione finora
- Dental Considerations For Patients With Lupus ErythematosusDocumento55 pagineDental Considerations For Patients With Lupus ErythematosusPhyo Ko KoNessuna valutazione finora
- Rheumatoid Arthritis Nursing Care PlanDocumento22 pagineRheumatoid Arthritis Nursing Care PlanLorelyn Santos Corpuz100% (1)
- Rheumatology: Osteoarthritis Rheumatoid Arthritis: Dr. Meg-Angela Christi AmoresDocumento25 pagineRheumatology: Osteoarthritis Rheumatoid Arthritis: Dr. Meg-Angela Christi AmoresNinaNessuna valutazione finora
- Management of Rheumatoid ArthritisDocumento44 pagineManagement of Rheumatoid ArthritisDeepak NemaniNessuna valutazione finora
- Arthritis: Dr.A.Prakash M.S. Orthopedics Fellow in Trauma and Arthroplasty. Ortho Life Hospital, ErodeDocumento36 pagineArthritis: Dr.A.Prakash M.S. Orthopedics Fellow in Trauma and Arthroplasty. Ortho Life Hospital, ErodemrkasprakashNessuna valutazione finora
- Resident Guide To Pediatric Rheumatology 2011Documento61 pagineResident Guide To Pediatric Rheumatology 2011Ana HinicNessuna valutazione finora
- Rheumatoid ArthritisDocumento23 pagineRheumatoid Arthritisfabunmiopeyemiv23Nessuna valutazione finora
- New Text DocumentDocumento1 paginaNew Text DocumentPande Indra PremanaNessuna valutazione finora
- Study Report DHF and Dengue Fever, Untuk MuatDocumento13 pagineStudy Report DHF and Dengue Fever, Untuk MuatPande Indra PremanaNessuna valutazione finora
- Toxoplasmosis in PregnancyDocumento13 pagineToxoplasmosis in PregnancyPande Indra PremanaNessuna valutazione finora
- 6 ImunoTechniques 2012Documento32 pagine6 ImunoTechniques 2012Pande Indra PremanaNessuna valutazione finora
- Alimentary Disorders: Symptoms, Tests, and DiagnosesDocumento1 paginaAlimentary Disorders: Symptoms, Tests, and DiagnosesPande Indra PremanaNessuna valutazione finora
- 2 Organel LinaDocumento34 pagine2 Organel LinaMade WidianantaraNessuna valutazione finora
- Upper Alimentary Histology-2012Documento23 pagineUpper Alimentary Histology-2012Pande Indra PremanaNessuna valutazione finora
- Diagnosis Dan Tatalaksana: Nyoman PurwadiDocumento26 pagineDiagnosis Dan Tatalaksana: Nyoman PurwadiPande Indra PremanaNessuna valutazione finora
- Learning Task Alimentary: Self AssessmentDocumento1 paginaLearning Task Alimentary: Self AssessmentPande Indra PremanaNessuna valutazione finora
- Upper Alimentary Histology-2012Documento23 pagineUpper Alimentary Histology-2012Pande Indra PremanaNessuna valutazione finora
- 8 Rinitis Alergi Eng VersionDocumento24 pagine8 Rinitis Alergi Eng VersionPande Indra PremanaNessuna valutazione finora
- Diagnosis and Management of AmebiasisDocumento9 pagineDiagnosis and Management of AmebiasisPande Indra PremanaNessuna valutazione finora
- General Principles Physical Exam GuideDocumento43 pagineGeneral Principles Physical Exam GuidePande Indra PremanaNessuna valutazione finora
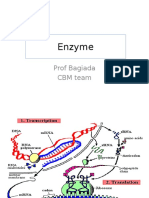
- Enzyme: Prof Bagiada CBM TeamDocumento30 pagineEnzyme: Prof Bagiada CBM TeamPande Indra PremanaNessuna valutazione finora
- 9 The Balinese TradmedCAMDocumento43 pagine9 The Balinese TradmedCAMPande Indra PremanaNessuna valutazione finora
- Uroflowmetry ProcedureDocumento1 paginaUroflowmetry ProcedurePande Indra PremanaNessuna valutazione finora
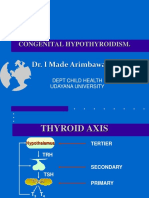
- 19 Congenital HipotiroidDocumento21 pagine19 Congenital HipotiroidPande Indra PremanaNessuna valutazione finora
- AA Gde Oka Sub-Lab/SMF Urologi FK - UNUD/RSUP Sanglah DenpasarDocumento26 pagineAA Gde Oka Sub-Lab/SMF Urologi FK - UNUD/RSUP Sanglah DenpasarPande Indra PremanaNessuna valutazione finora
- 17 Adrenal GlandDocumento33 pagine17 Adrenal GlandPande Indra PremanaNessuna valutazione finora
- Measurements of Morbidity and Mortality in A Population & Source of ErrorDocumento38 pagineMeasurements of Morbidity and Mortality in A Population & Source of ErrorPande Indra PremanaNessuna valutazione finora
- Pathogenesis of Bacterial Infection Sem 3Documento46 paginePathogenesis of Bacterial Infection Sem 3Sheryl ElitaNessuna valutazione finora
- 2 Total Ergonomic ApproachDocumento25 pagine2 Total Ergonomic ApproachPande Indra PremanaNessuna valutazione finora
- Doraemon Cartoon Summary: Nobita's Cat Robot Friend From The FutureDocumento3 pagineDoraemon Cartoon Summary: Nobita's Cat Robot Friend From The FuturePande Indra PremanaNessuna valutazione finora
- Describe of Definition of PolypharmacyDocumento1 paginaDescribe of Definition of PolypharmacyPande Indra PremanaNessuna valutazione finora
- Measurements of Morbidity and Mortality in A Population & Source of ErrorDocumento38 pagineMeasurements of Morbidity and Mortality in A Population & Source of ErrorPande Indra PremanaNessuna valutazione finora
- Genetic Counseling and Prenatal DiagnosisDocumento13 pagineGenetic Counseling and Prenatal DiagnosisPande Indra Premana100% (1)
- Treatment of Viral InfectionDocumento33 pagineTreatment of Viral InfectionPande Indra PremanaNessuna valutazione finora
- Achondroplasia Emedicine DKKDocumento29 pagineAchondroplasia Emedicine DKKPande Indra PremanaNessuna valutazione finora
- 19 Congenital HipotiroidDocumento21 pagine19 Congenital HipotiroidPande Indra PremanaNessuna valutazione finora
- 24.postpartum Period-Physiological Changes in The MotherDocumento16 pagine24.postpartum Period-Physiological Changes in The MotherHem KumariNessuna valutazione finora
- Liquid Out, Temperature 25.5 °C Tube: M/gs P / WDocumento7 pagineLiquid Out, Temperature 25.5 °C Tube: M/gs P / WGianra RadityaNessuna valutazione finora
- Railway Airport Docks and HarbourDocumento21 pagineRailway Airport Docks and HarbourvalarmathibalanNessuna valutazione finora
- Discuss The Challenges For Firms To Operate in The Hard-Boiled Confectionery Market in India?Documento4 pagineDiscuss The Challenges For Firms To Operate in The Hard-Boiled Confectionery Market in India?harryNessuna valutazione finora
- HVCCI UPI Form No. 3 Summary ReportDocumento2 pagineHVCCI UPI Form No. 3 Summary ReportAzumi AyuzawaNessuna valutazione finora
- Monster of The Week Tome of Mysteries PlaybooksDocumento10 pagineMonster of The Week Tome of Mysteries PlaybooksHyperLanceite XNessuna valutazione finora
- Lyceum of The Philippines University Cavite Potential of Peanut Hulls As An Alternative Material On Making Biodegradable PlasticDocumento13 pagineLyceum of The Philippines University Cavite Potential of Peanut Hulls As An Alternative Material On Making Biodegradable PlasticJayr Mercado0% (1)
- Tetracyclines: Dr. Md. Rageeb Md. Usman Associate Professor Department of PharmacognosyDocumento21 pagineTetracyclines: Dr. Md. Rageeb Md. Usman Associate Professor Department of PharmacognosyAnonymous TCbZigVqNessuna valutazione finora
- Math 202: Di Fferential Equations: Course DescriptionDocumento2 pagineMath 202: Di Fferential Equations: Course DescriptionNyannue FlomoNessuna valutazione finora
- Rotary Twin Scew Brochure UK HRDocumento20 pagineRotary Twin Scew Brochure UK HRNguyễn Hữu DũngNessuna valutazione finora
- Design of Fixed Column Base JointsDocumento23 pagineDesign of Fixed Column Base JointsLanfranco CorniaNessuna valutazione finora
- India - Wikipedia, The Free EncyclopediaDocumento40 pagineIndia - Wikipedia, The Free EncyclopediaPrashanth KrishNessuna valutazione finora
- CANAL (T) Canal Soth FloridaDocumento115 pagineCANAL (T) Canal Soth FloridaMIKHA2014Nessuna valutazione finora
- 40 26Documento3 pagine40 26Maxi452Nessuna valutazione finora
- Oral Nutrition Support NotesDocumento28 pagineOral Nutrition Support Notesleemon.mary.alipao8695Nessuna valutazione finora
- Caterpillar Ep15krtDocumento37 pagineCaterpillar Ep15krtIvan MajikNessuna valutazione finora
- Ricoh 4055 PDFDocumento1.280 pagineRicoh 4055 PDFPham Nguyen Hoang Minh100% (1)
- Direct From: 1St Quarter 2020Documento23 pagineDirect From: 1St Quarter 2020JeanNessuna valutazione finora
- APLICACIONES PARA AUTOS Y CARGA LIVIANADocumento50 pagineAPLICACIONES PARA AUTOS Y CARGA LIVIANApancho50% (2)
- SB Z Audio2Documento2 pagineSB Z Audio2api-151773256Nessuna valutazione finora
- Material and Energy Balance: PN Husna Binti ZulkiflyDocumento108 pagineMaterial and Energy Balance: PN Husna Binti ZulkiflyFiras 01Nessuna valutazione finora
- Evolutionary PsychologyDocumento10 pagineEvolutionary PsychologyShreya MadheswaranNessuna valutazione finora
- Seed SavingDocumento21 pagineSeed SavingElectroPig Von FökkenGrüüven100% (2)
- Philippines' Legal Basis for Claims in South China SeaDocumento38 paginePhilippines' Legal Basis for Claims in South China SeaGeeNessuna valutazione finora
- Casio AP-80R Service ManualDocumento41 pagineCasio AP-80R Service ManualEngkiong Go100% (1)
- Letter of MotivationDocumento4 pagineLetter of Motivationjawad khalidNessuna valutazione finora
- Private Schools Provide Better EducationDocumento2 paginePrivate Schools Provide Better EducationcitraNessuna valutazione finora
- Lightwave Maya 3D TutorialsDocumento8 pagineLightwave Maya 3D TutorialsrandfranNessuna valutazione finora
- Awakening The MindDocumento21 pagineAwakening The MindhhhumNessuna valutazione finora
- European GMP Annex 1 - 2008 Edition - 'Pmeasuring'Documento3 pagineEuropean GMP Annex 1 - 2008 Edition - 'Pmeasuring'Khairul AnwarNessuna valutazione finora