Potrebbero piacerti anche
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsDa EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNessuna valutazione finora
- Solutions to Diabetes and Hypoglycemia (Translated): How to prevent and get rid of it in a natural way, without resorting to medicines but adopting a correct way of lifeDa EverandSolutions to Diabetes and Hypoglycemia (Translated): How to prevent and get rid of it in a natural way, without resorting to medicines but adopting a correct way of lifeNessuna valutazione finora
- #3 Pancreatic Hormones & Antidiabetic Drugs 14 PDFDocumento14 pagine#3 Pancreatic Hormones & Antidiabetic Drugs 14 PDFOmar BasimNessuna valutazione finora
- Introduction of Animal HormoneDocumento6 pagineIntroduction of Animal HormonePC BUGNessuna valutazione finora
- Physiology of Diabetes: Dr. Solomon Sathishkumar. MDDocumento36 paginePhysiology of Diabetes: Dr. Solomon Sathishkumar. MDKhaled LajmiNessuna valutazione finora
- All Types of InsulinDocumento18 pagineAll Types of Insulinali mohammedNessuna valutazione finora
- Hormonal Secretion of PancreasDocumento17 pagineHormonal Secretion of PancreasNazia WasimNessuna valutazione finora
- Anti-Hyperglycaemic DrugsDocumento53 pagineAnti-Hyperglycaemic DrugsNathanNessuna valutazione finora
- Physio 7Documento12 paginePhysio 7amjadNessuna valutazione finora
- Diabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManDocumento66 pagineDiabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManNora Budina Abdinesia RitongaNessuna valutazione finora
- Dr. Solomon Sathishkumar, MD Department of Physiology Christian Medical College Vellore, IndiaDocumento48 pagineDr. Solomon Sathishkumar, MD Department of Physiology Christian Medical College Vellore, IndiaKrairat KomdeeNessuna valutazione finora
- Carbohydrate - MetabolismDocumento12 pagineCarbohydrate - MetabolismShimmering MoonNessuna valutazione finora
- Group 3 Concepcion Contacto Cordero Cornejo Cornell Cortez CruzDocumento62 pagineGroup 3 Concepcion Contacto Cordero Cornejo Cornell Cortez CruzConcepcion Kevin ChuckNessuna valutazione finora
- INSULINDocumento24 pagineINSULINAreen Emilia Faizlukman JerryNessuna valutazione finora
- Diabetes MellituspptxDocumento69 pagineDiabetes Mellituspptxnuguitnorelyn30Nessuna valutazione finora
- Diabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManDocumento66 pagineDiabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManyuliNessuna valutazione finora
- Diabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManDocumento66 pagineDiabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManElvis J. DavisNessuna valutazione finora
- What Are The Cellular and Molecular Actions of Insulin?Documento13 pagineWhat Are The Cellular and Molecular Actions of Insulin?Elle ReyesNessuna valutazione finora
- Homeostasis and The Regulation of Blood GlucoseDocumento7 pagineHomeostasis and The Regulation of Blood GlucoseElgin SammonsNessuna valutazione finora
- Diabetes Mellitus: Regulation of Blood GlucoseDocumento65 pagineDiabetes Mellitus: Regulation of Blood GlucoseReggae BautistaNessuna valutazione finora
- Presented by DR Ashish Sharma Guided by DR Meena PatelDocumento74 paginePresented by DR Ashish Sharma Guided by DR Meena PatelAndrew Surya Putra SccNessuna valutazione finora
- MBS2-K7-Pharmacology of Endocrine PancreasDocumento55 pagineMBS2-K7-Pharmacology of Endocrine PancreasZoga Pratantia TohariNessuna valutazione finora
- Common Endocrine Disorders: Iril I. Panes, RN, MANDocumento63 pagineCommon Endocrine Disorders: Iril I. Panes, RN, MANJona Phie Domingo MonteroNessuna valutazione finora
- Endo Pancrease ElhDocumento27 pagineEndo Pancrease Elhodiodi57Nessuna valutazione finora
- Lesson 15: Drugs For Diabetes: Introduction (ILO-1 - 2)Documento38 pagineLesson 15: Drugs For Diabetes: Introduction (ILO-1 - 2)Ralp ManglicmotNessuna valutazione finora
- Diabetes MellitusDocumento6 pagineDiabetes Mellitusmar_ouqNessuna valutazione finora
- Anti-Diabetic Drugs Part A-2Documento35 pagineAnti-Diabetic Drugs Part A-2rimsha waseemNessuna valutazione finora
- InsulinDocumento6 pagineInsulinAmbroseNessuna valutazione finora
- Diabetes MellitusDocumento16 pagineDiabetes MellitusApril Joy V. QuinoNessuna valutazione finora
- Metabolisme Insulin Dan GlukagonDocumento7 pagineMetabolisme Insulin Dan GlukagonDinda saylaNessuna valutazione finora
- Diabetes Mellitus Type 11Documento44 pagineDiabetes Mellitus Type 11MARICRIS NEBIARNessuna valutazione finora
- Diabetes MellitusDocumento13 pagineDiabetes MellitusGeoffreyNessuna valutazione finora
- Insulin: The Structure of Insulin. The Left Side Is A Space-Filling Model of The InsulinDocumento21 pagineInsulin: The Structure of Insulin. The Left Side Is A Space-Filling Model of The Insulinsuho exoNessuna valutazione finora
- The Insulin Receptor and Mechanism of ActionDocumento5 pagineThe Insulin Receptor and Mechanism of ActionMonica AbabeiNessuna valutazione finora
- Why Is The Brain The Most Important Consumer of Glucose?Documento11 pagineWhy Is The Brain The Most Important Consumer of Glucose?PojangNessuna valutazione finora
- Exam Part IIDocumento13 pagineExam Part IIlpirman05Nessuna valutazione finora
- Effect of Insulin On Carbohydrate MetabolismDocumento3 pagineEffect of Insulin On Carbohydrate MetabolismfrnksusNessuna valutazione finora
- 04 Physiology of The Pancreas PDFDocumento66 pagine04 Physiology of The Pancreas PDFMonesa Christy VillanuevaNessuna valutazione finora
- Pacreas and Gonads - TILLESDocumento7 paginePacreas and Gonads - TILLESAna Marie D. BorjaNessuna valutazione finora
- Pancreas PancreasDocumento18 paginePancreas PancreasZzeba KhanNessuna valutazione finora
- Diabetes Mellitus and Laboratory Tests of DiabetesDocumento24 pagineDiabetes Mellitus and Laboratory Tests of DiabetesturkiNessuna valutazione finora
- Tolentino BiochemDiabetesDocumento3 pagineTolentino BiochemDiabetesjelyn suarezNessuna valutazione finora
- InsulinDocumento50 pagineInsulinTandin SonamNessuna valutazione finora
- Diabetes KetoacidosisDocumento35 pagineDiabetes KetoacidosisdaniejayanandNessuna valutazione finora
- Biochemistry Lecture 8 Final PPT - B&WDocumento35 pagineBiochemistry Lecture 8 Final PPT - B&Wsamyu827Nessuna valutazione finora
- CarbohydratesDocumento37 pagineCarbohydratesMthandeni KhumaloNessuna valutazione finora
- Pancreas 2021Documento32 paginePancreas 2021Dr. AliNessuna valutazione finora
- Insulin Storage and ReleaseDocumento18 pagineInsulin Storage and ReleaseAditya KotamrajuNessuna valutazione finora
- Insulin and Oral Hypoglycemic AgentsDocumento27 pagineInsulin and Oral Hypoglycemic Agentsapi-19916399100% (1)
- Insulin and The Oral HypoglycemicsDocumento9 pagineInsulin and The Oral HypoglycemicsHasibNessuna valutazione finora
- Endocrine Pancreas & Fuel Homeostasis: Learning ObjectivesDocumento7 pagineEndocrine Pancreas & Fuel Homeostasis: Learning ObjectivesEmmanuel NhandaraNessuna valutazione finora
- Blood Sugar Reg-WPS OfficeDocumento8 pagineBlood Sugar Reg-WPS Officetanjidul islamNessuna valutazione finora
- Human Biology (Biologi Manuasia) : Prof Madya Dr. Mohamad Aziz DollahDocumento29 pagineHuman Biology (Biologi Manuasia) : Prof Madya Dr. Mohamad Aziz DollahQisNani NorainiNessuna valutazione finora
- Endocrine Week 2Documento18 pagineEndocrine Week 2Clauvinna Lie FiscaNessuna valutazione finora
- Path Phys3Documento73 paginePath Phys3Наталія Вікторівна ДавиденкоNessuna valutazione finora
- InsulinDocumento19 pagineInsulinglobalaffairzNessuna valutazione finora
- UNIT - IV Endocrine Diseases, Sub Unit 4.2 Diabetes Mellitus - Etiology and Pathogenesis of Diabetes - Clinical Manifestations of The Disease - Management of The Disease - Complications of Diabetes.Documento40 pagineUNIT - IV Endocrine Diseases, Sub Unit 4.2 Diabetes Mellitus - Etiology and Pathogenesis of Diabetes - Clinical Manifestations of The Disease - Management of The Disease - Complications of Diabetes.reza dehghaniNessuna valutazione finora
- Chemical Pathology 5 - HypoglycaemiaDocumento10 pagineChemical Pathology 5 - HypoglycaemiaaNessuna valutazione finora
- Metabolism Interaction and Hormone Regulation.Documento81 pagineMetabolism Interaction and Hormone Regulation.fikaduNessuna valutazione finora
- Anaphy and PathophyDocumento6 pagineAnaphy and PathophyMagdaraog Gabrielle A.Nessuna valutazione finora
- Orthopaedic RadiographyDocumento8 pagineOrthopaedic RadiographyMarie Elexis RevillezaNessuna valutazione finora
- L1 2015 Nervous SystemDocumento6 pagineL1 2015 Nervous SystemMarie Elexis RevillezaNessuna valutazione finora
- Biological Effects of Androgen On Male and FemaleDocumento22 pagineBiological Effects of Androgen On Male and FemaleMarie Elexis RevillezaNessuna valutazione finora
- Rizal From The Perspective of Filipino Intellectuals Rizal's Political ThoughtDocumento20 pagineRizal From The Perspective of Filipino Intellectuals Rizal's Political ThoughtMarie Elexis RevillezaNessuna valutazione finora
- Armed Self Defense - Arnis: Physical Education and Health 12Documento19 pagineArmed Self Defense - Arnis: Physical Education and Health 12Kobe CruzNessuna valutazione finora
- Project QuestionairreDocumento3 pagineProject QuestionairreRuhee JivaniNessuna valutazione finora
- 30 MethodsDocumento8 pagine30 Methodspapa mote hai81% (32)
- Sword HandDocumento4 pagineSword HandjckhouryNessuna valutazione finora
- BFA Nominee ListDocumento2 pagineBFA Nominee ListBernews AdmnNessuna valutazione finora
- Kit de Montaje para CilindrosDocumento2 pagineKit de Montaje para CilindrossandraNessuna valutazione finora
- Descent 2nd Edition - The Shadow RuneDocumento44 pagineDescent 2nd Edition - The Shadow RuneJames Eisert100% (1)
- Catalogo Mecanico Electrico JLG 80 HX+6 InglesDocumento538 pagineCatalogo Mecanico Electrico JLG 80 HX+6 Inglescristian faundes100% (1)
- Gracie Jiu-JitsuDocumento52 pagineGracie Jiu-JitsuKarina HuapayaNessuna valutazione finora
- A Cold Night in Klettwitz PDFDocumento5 pagineA Cold Night in Klettwitz PDFMichael MerlinNessuna valutazione finora
- Front Squat - CrossFit Training GuideDocumento2 pagineFront Squat - CrossFit Training GuideKarim HaridiNessuna valutazione finora
- Mwos Sunday FixtureDocumento22 pagineMwos Sunday FixtureMaxwell ManyangaNessuna valutazione finora
- The Duggins-Briggs Fortune Telling Card MeaningsDocumento1 paginaThe Duggins-Briggs Fortune Telling Card Meaningssunoflight396100% (3)
- Soccer Formation Lineup Sheet 11v11 4132Documento1 paginaSoccer Formation Lineup Sheet 11v11 4132داود ميلاحNessuna valutazione finora
- Bet Slip 10Documento4 pagineBet Slip 10Jordi NaibahoNessuna valutazione finora
- Chain Sling Toolbox TalkDocumento6 pagineChain Sling Toolbox Talkfathul syaafNessuna valutazione finora
- R000072Documento97 pagineR000072Andres VillagomezNessuna valutazione finora
- DECATHLONDocumento35 pagineDECATHLONHanna Relator Dolor100% (2)
- Serial Number: XT 85xt - Case Skid Steer Loader (09/97 - 12/05) 06 - Power Train 06-12 - Pump, Tandem, Cylinder Block and PistonDocumento3 pagineSerial Number: XT 85xt - Case Skid Steer Loader (09/97 - 12/05) 06 - Power Train 06-12 - Pump, Tandem, Cylinder Block and PistonSebastián Fernando Canul MendezNessuna valutazione finora
- Recreational ActivitiesDocumento8 pagineRecreational ActivitiesChristian ReposarNessuna valutazione finora
- Safety & Maintenance Checklist Underground Trucks PDFDocumento1 paginaSafety & Maintenance Checklist Underground Trucks PDFGustavoNessuna valutazione finora
- RpiDocumento4 pagineRpiEVENessuna valutazione finora
- Traditional Games in The PhilippinesDocumento47 pagineTraditional Games in The Philippinesagustin86% (7)
- Basketball Defense Syracuse 2-3 ZoneDocumento3 pagineBasketball Defense Syracuse 2-3 ZoneEmmanuel SaravasNessuna valutazione finora
- Hose Management Guide: SN: Agc Lines Group - AttachmentDocumento42 pagineHose Management Guide: SN: Agc Lines Group - AttachmentJose luis Consuegra100% (1)
- (Kalmar: DCE80-45E7 10 61Documento12 pagine(Kalmar: DCE80-45E7 10 61cutoNessuna valutazione finora
- Great Yoga PDFDocumento24 pagineGreat Yoga PDFGuyenne NguyenNessuna valutazione finora
- Adele - Rolling in The Deep - 1.0Documento1 paginaAdele - Rolling in The Deep - 1.0Jennifer PorterNessuna valutazione finora
- Python Dataframe Assignment No 1 - AnswerkeyDocumento7 paginePython Dataframe Assignment No 1 - AnswerkeyAnni KumarNessuna valutazione finora
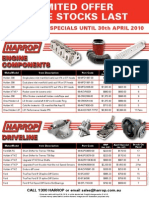
- April Special Flyer v4Documento1 paginaApril Special Flyer v4Harrop_salesNessuna valutazione finora