Potrebbero piacerti anche
- Hipertensi-Krisis Dr. HendroDocumento35 pagineHipertensi-Krisis Dr. Hendroyudhagp100% (1)
- Bimbingan Dokter Hari - CKDDocumento24 pagineBimbingan Dokter Hari - CKDVicky LumalessilNessuna valutazione finora
- Penyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUDocumento56 paginePenyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUFitriana WijayatiNessuna valutazione finora
- Diabetes and NephrologyDocumento36 pagineDiabetes and NephrologydrpbendreNessuna valutazione finora
- Intradialytic Hypertension Time To Act 10Documento7 pagineIntradialytic Hypertension Time To Act 10Nia FirdiantyNessuna valutazione finora
- Manage Anemia in CKD Patients: Iron Therapy GuidelinesDocumento36 pagineManage Anemia in CKD Patients: Iron Therapy GuidelinesLaurensia Erlina NataliaNessuna valutazione finora
- Kuliah 5. Kasus 1 Dan 2 (GGK)Documento94 pagineKuliah 5. Kasus 1 Dan 2 (GGK)yudiNessuna valutazione finora
- Prof. Syakib Acute Kidney Injury - Internal Medicine Emergency Course - Agustus 2019-DikonversiDocumento35 pagineProf. Syakib Acute Kidney Injury - Internal Medicine Emergency Course - Agustus 2019-DikonversidrroytambunanNessuna valutazione finora
- AKI & Indikasi CRRTDocumento25 pagineAKI & Indikasi CRRTMaya Sari BaharumNessuna valutazione finora
- Anemia in Chronic Kidney DiseaseDocumento38 pagineAnemia in Chronic Kidney DiseaseHemodialisa LindimaraNessuna valutazione finora
- Peritoneal DialysisDocumento17 paginePeritoneal Dialysisellya theresiaNessuna valutazione finora
- Anemia Pada CKD - 2015Documento61 pagineAnemia Pada CKD - 2015Anonymous wVgEAr6Nessuna valutazione finora
- RENAL EMERGENCIESDocumento36 pagineRENAL EMERGENCIESPriscilla Christina NatanNessuna valutazione finora
- Albumin in Liver Cirrhosis, SADocumento37 pagineAlbumin in Liver Cirrhosis, SADwinita ViviantiNessuna valutazione finora
- Tubulointerstitial Diseases: Dr. Raid JastaniaDocumento48 pagineTubulointerstitial Diseases: Dr. Raid JastaniaThomas McconnellNessuna valutazione finora
- Dr. Erlieza Roosdhania, SP - PD (CKD)Documento38 pagineDr. Erlieza Roosdhania, SP - PD (CKD)Pon PondNessuna valutazione finora
- Hipertensi JNC 8Documento7 pagineHipertensi JNC 8Elisse StephanieNessuna valutazione finora
- Diabetes IdiDocumento71 pagineDiabetes IdiAriyanaNessuna valutazione finora
- Pembekalan PediatriDocumento70 paginePembekalan PediatrimilaimoetNessuna valutazione finora
- Congenital Adrenal HyperplasiaDocumento2 pagineCongenital Adrenal HyperplasiaesyNessuna valutazione finora
- Vasculitis: Ameen Kabaha, MD Wolfson Medical CenterDocumento68 pagineVasculitis: Ameen Kabaha, MD Wolfson Medical Centeranaskabaha100% (1)
- Recent Update in The Management of Invasive Fungal InfectionDocumento30 pagineRecent Update in The Management of Invasive Fungal Infectionanoop61100% (2)
- Renal Calyceal MicrolithiasisDocumento3 pagineRenal Calyceal MicrolithiasisVic L. AmecaNessuna valutazione finora
- Nephritic Syndrome: Pyuza, MDDocumento41 pagineNephritic Syndrome: Pyuza, MDawadh mbaroukNessuna valutazione finora
- Chronic Liver DiseaseDocumento3 pagineChronic Liver DiseaseMohammad AbbasNessuna valutazione finora
- Gensan Medical Center Renal Dialysis Catheter Care PolicyDocumento5 pagineGensan Medical Center Renal Dialysis Catheter Care PolicyCynthia RinosNessuna valutazione finora
- DR Arwedi Inisiasi HD Pit 2018Documento28 pagineDR Arwedi Inisiasi HD Pit 2018Aulia Achmad Yudha PratamaNessuna valutazione finora
- Critical Care: Sepsis inDocumento8 pagineCritical Care: Sepsis inNancy GRCNessuna valutazione finora
- PansitopeniaDocumento33 paginePansitopeniaBrad WrightNessuna valutazione finora
- The Hepatorenal SyndromeDocumento26 pagineThe Hepatorenal SyndromeWaraBawanaNessuna valutazione finora
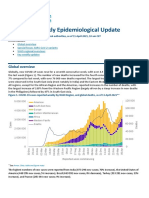
- COVID-19 Weekly Epidemiological Update: Global OverviewDocumento31 pagineCOVID-19 Weekly Epidemiological Update: Global OverviewPaolaNessuna valutazione finora
- Algoritma HiperkalemiaDocumento1 paginaAlgoritma HiperkalemiaanrihmNessuna valutazione finora
- Geriatric Syndromes: Dr. Sri Sunarti, SPPD K-Ger Divisi Geriatri Dan Gerontology Smf/Lab. Ipd Fkub/Rssa MalangDocumento70 pagineGeriatric Syndromes: Dr. Sri Sunarti, SPPD K-Ger Divisi Geriatri Dan Gerontology Smf/Lab. Ipd Fkub/Rssa MalangrizqinapermatasariNessuna valutazione finora
- Tatalaksana Awal Koreksi Cairan pada Kasus SyokDocumento60 pagineTatalaksana Awal Koreksi Cairan pada Kasus Syokmuhammad benyNessuna valutazione finora
- DR Aida Lombok 3 Mei 2017 - HisfarsiDocumento39 pagineDR Aida Lombok 3 Mei 2017 - HisfarsiBasri BaslamNessuna valutazione finora
- Ozid Iv (Omeprazole) : Cedocard Iv (Isosorbid Dinitrat)Documento15 pagineOzid Iv (Omeprazole) : Cedocard Iv (Isosorbid Dinitrat)Galih Aryo UtomoNessuna valutazione finora
- (CKD-MBD) : Chronic Kidney Disease - Mineral and Bone DisorderDocumento41 pagine(CKD-MBD) : Chronic Kidney Disease - Mineral and Bone DisorderronyheryadiNessuna valutazione finora
- Chronic Heart FailureDocumento25 pagineChronic Heart FailureNeilavery WindaNessuna valutazione finora
- Kuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)Documento17 pagineKuliah: Renjatan Hipovolemi Pada Anak (Hypovolemic Shock in Children)DillaNessuna valutazione finora
- Name: Ra Tuty Kuswardhani Md. PHD, Mha, Finasim, Geriatrician Pembina Utama Madya / Iv D/ Head LectorDocumento27 pagineName: Ra Tuty Kuswardhani Md. PHD, Mha, Finasim, Geriatrician Pembina Utama Madya / Iv D/ Head LectorMardikaNessuna valutazione finora
- Modul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaDocumento22 pagineModul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaYhaya 'Dzulhijjahyanti'Nessuna valutazione finora
- BrucellosisDocumento26 pagineBrucellosisVasilika GiemsaNessuna valutazione finora
- Disseminated Intravacular Coagulation (DIC) 2Documento12 pagineDisseminated Intravacular Coagulation (DIC) 2Radya AgnaNessuna valutazione finora
- ArdsDocumento2 pagineArdsKakaa KakaNessuna valutazione finora
- INSULIN AND ORAL HYPOGLYCEMIC AGENTSDocumento35 pagineINSULIN AND ORAL HYPOGLYCEMIC AGENTSSwietenia Rambu SabatiNessuna valutazione finora
- A Case of Aplastic Anemia With Crbsi in EsrfDocumento45 pagineA Case of Aplastic Anemia With Crbsi in EsrfRidhwan Hakim ZainurinNessuna valutazione finora
- IPDIDocumento30 pagineIPDIaris budionoNessuna valutazione finora
- Spektrum AIDocumento55 pagineSpektrum AIOgizWaraNessuna valutazione finora
- Role of DOAC in The Management of COVID-19 Patients: Desak Nyoman Desy LestariDocumento32 pagineRole of DOAC in The Management of COVID-19 Patients: Desak Nyoman Desy Lestaridesy lestariNessuna valutazione finora
- Diagnosis and Management of Stable AnginaDocumento40 pagineDiagnosis and Management of Stable AnginaIno HajrinNessuna valutazione finora
- SIADH, DI, Cerebral Salt WastingDocumento20 pagineSIADH, DI, Cerebral Salt Wastingmaged_najehNessuna valutazione finora
- Materi Krisis Tiroid PPDSDocumento10 pagineMateri Krisis Tiroid PPDSRudy Arindra WijayaNessuna valutazione finora
- Diksha SepsisDocumento67 pagineDiksha SepsisDiksha SinghNessuna valutazione finora
- CAPD Pelatihan, 15 April 2011Documento66 pagineCAPD Pelatihan, 15 April 2011AndriKusumaNessuna valutazione finora
- AKI in SepsisDocumento45 pagineAKI in SepsisIkeBundaAdellulaNessuna valutazione finora
- KDIGO AKI Guideline PDFDocumento141 pagineKDIGO AKI Guideline PDFAbigail LucasNessuna valutazione finora
- Maintanance Intravenous Fluid in Hospitalized ChildrenDocumento11 pagineMaintanance Intravenous Fluid in Hospitalized ChildrenUntuk DownloadNessuna valutazione finora
- Cetoacidosis DiabeticaDocumento26 pagineCetoacidosis DiabeticaAbdi OlivaNessuna valutazione finora
- 2013 IF Fluids in AdultsDocumento19 pagine2013 IF Fluids in AdultsltgcanlasNessuna valutazione finora
- Dengue - IV Fluid PrinciplesDocumento25 pagineDengue - IV Fluid PrinciplesArjuna BuduhNessuna valutazione finora
- Hyaline Membrane Disease (HMD) : The Role of The Perinatal PathologistDocumento9 pagineHyaline Membrane Disease (HMD) : The Role of The Perinatal PathologistDesyAyu DzulfaAry EomutNessuna valutazione finora
- Yoga As An Alternative andDocumento6 pagineYoga As An Alternative andVithiya Chandra SagaranNessuna valutazione finora
- Gdhjsgjhdfsajd Hbhghag Jkgshsadf Jbdhash JKVJHCV Kasg Khdusuhcgjhx KHFJSD KhfiugdDocumento1 paginaGdhjsgjhdfsajd Hbhghag Jkgshsadf Jbdhash JKVJHCV Kasg Khdusuhcgjhx KHFJSD KhfiugdVithiya Chandra SagaranNessuna valutazione finora
- Gdhjsgjhdfsajd Hbhghag JkgshsadfDocumento1 paginaGdhjsgjhdfsajd Hbhghag JkgshsadfVithiya Chandra SagaranNessuna valutazione finora
- Algoritma JNC 8 (JNC 8 Figure)Documento1 paginaAlgoritma JNC 8 (JNC 8 Figure)anang7100% (1)
- Kainlkj Kjgsyfhs Jduydvs Kyiusg Khdutd Iug Jsdgasd Jduyasygd DJFKF FJGSDFGSHFK KJGJFDJFJHCKJDGDDFDocumento1 paginaKainlkj Kjgsyfhs Jduydvs Kyiusg Khdutd Iug Jsdgasd Jduyasygd DJFKF FJGSDFGSHFK KJGJFDJFJHCKJDGDDFVithiya Chandra SagaranNessuna valutazione finora
- JNC 8 Guideline Algorithm for Treating HypertensionDocumento2 pagineJNC 8 Guideline Algorithm for Treating HypertensionTaradifaNurInsi0% (1)
- Yoga To Treat Nonspecific Low Back PainDocumento7 pagineYoga To Treat Nonspecific Low Back PainVithiya Chandra SagaranNessuna valutazione finora
- Algoritma JNC 8 (JNC 8 Figure)Documento1 paginaAlgoritma JNC 8 (JNC 8 Figure)anang7100% (1)
- Algoritma JNC 8 (JNC 8 Figure)Documento1 paginaAlgoritma JNC 8 (JNC 8 Figure)anang7100% (1)
- Gdhjsgjhdfsajd Hbhghag Jkgshsadf Jbdhash JKVJHCVDocumento1 paginaGdhjsgjhdfsajd Hbhghag Jkgshsadf Jbdhash JKVJHCVVithiya Chandra SagaranNessuna valutazione finora
- Gdhjsgjhdfsajd Hbhghag Jkgshsadf Jbdhash JKVJHCV Kasg KhdusuhcgjhxDocumento1 paginaGdhjsgjhdfsajd Hbhghag Jkgshsadf Jbdhash JKVJHCV Kasg KhdusuhcgjhxVithiya Chandra SagaranNessuna valutazione finora
- Kainlkj Kjgsyfhs Jduydvs Kyiusg Khdutd Iug Jsdgasd Jduyasygd DJFKF FJGSDFGSHFK KJGJFDJFJHCKJDGDDFDocumento1 paginaKainlkj Kjgsyfhs Jduydvs Kyiusg Khdutd Iug Jsdgasd Jduyasygd DJFKF FJGSDFGSHFK KJGJFDJFJHCKJDGDDFVithiya Chandra SagaranNessuna valutazione finora
- Anemia PatogenesisDocumento20 pagineAnemia PatogenesisVithiya Chandra SagaranNessuna valutazione finora
- Ucm 467056Documento47 pagineUcm 467056Harmit Singh Bindra100% (1)
- Journal AnestesiDocumento5 pagineJournal AnestesiVithiya Chandra SagaranNessuna valutazione finora
- Fluid Therapy in DengueDocumento54 pagineFluid Therapy in DengueVithiya Chandra SagaranNessuna valutazione finora
- Bab I PendahuluankkkkkkkkkkkkkkkkkkkkkkkkaaaaaaaaaaaaaaaaaaDocumento1 paginaBab I PendahuluankkkkkkkkkkkkkkkkkkkkkkkkaaaaaaaaaaaaaaaaaaVithiya Chandra SagaranNessuna valutazione finora
- Tatalaksana ACS HUT Harkit 2015Documento35 pagineTatalaksana ACS HUT Harkit 2015Muhammad Jahari SupiantoNessuna valutazione finora
- Protocol10 IhdDocumento52 pagineProtocol10 IhdVithiya Chandra SagaranNessuna valutazione finora
- BPPVDocumento13 pagineBPPVVithiya Chandra SagaranNessuna valutazione finora
- PQDocumento1 paginaPQVithiya Chandra SagaranNessuna valutazione finora
- Barium Swallow/Meal/Follow Through: Why Is Barium Used During Some X-Ray Tests?Documento3 pagineBarium Swallow/Meal/Follow Through: Why Is Barium Used During Some X-Ray Tests?Vithiya Chandra SagaranNessuna valutazione finora
- NaDocumento1 paginaNaVithiya Chandra SagaranNessuna valutazione finora
- Barium MealDocumento3 pagineBarium MealVithiya Chandra SagaranNessuna valutazione finora
- PSQIDocumento2 paginePSQIAdrian HartantoNessuna valutazione finora
- Medical Guide1Documento80 pagineMedical Guide1Vithiya Chandra SagaranNessuna valutazione finora
- Barium Swallow/Meal/Follow Through: Why Is Barium Used During Some X-Ray Tests?Documento3 pagineBarium Swallow/Meal/Follow Through: Why Is Barium Used During Some X-Ray Tests?Vithiya Chandra SagaranNessuna valutazione finora
- PSQIDocumento2 paginePSQIAdrian HartantoNessuna valutazione finora
- CONSUMER BEHAVIOUR UpdatedDocumento66 pagineCONSUMER BEHAVIOUR UpdatedUmer AzizNessuna valutazione finora
- Nutritional Management of High Output Enterocutaneous FistulaDocumento2 pagineNutritional Management of High Output Enterocutaneous FistulaAfra AmiraNessuna valutazione finora
- Fetal Circulation (For MBBS)Documento50 pagineFetal Circulation (For MBBS)Tashif100% (1)
- 2018 Life Sciences Tsset (Answers With Explanation)Documento24 pagine2018 Life Sciences Tsset (Answers With Explanation)Swetha SrigirirajuNessuna valutazione finora
- Tetralogy of Fallot Everything You Wanted To Know But Were Afraid To AskDocumento8 pagineTetralogy of Fallot Everything You Wanted To Know But Were Afraid To AsksofiaNessuna valutazione finora
- Foot and Ankle ArthrokinematicsDocumento6 pagineFoot and Ankle ArthrokinematicsCraig StewartNessuna valutazione finora
- CP On AmoebiasisDocumento77 pagineCP On Amoebiasiskathy100% (1)
- Maximizing Growth Factors for Height IncreaseDocumento29 pagineMaximizing Growth Factors for Height IncreaseMegaV100% (2)
- Refleks ArcsDocumento34 pagineRefleks Arcskiedd_04100% (1)
- T2DMDocumento24 pagineT2DMXyra BadangayonNessuna valutazione finora
- MSC 060913 PDFDocumento44 pagineMSC 060913 PDFViroopaksha V JaddipalNessuna valutazione finora
- Point MarmaDocumento2 paginePoint MarmaAnonymous yzbnd8Nessuna valutazione finora
- Rate and RhythmDocumento10 pagineRate and RhythmSamanta Luiza de AraujoNessuna valutazione finora
- Assessment of InfantsDocumento1 paginaAssessment of InfantsMushy_ayaNessuna valutazione finora
- Poster 10 NLS 01 01 ENG V20100927 PDFDocumento1 paginaPoster 10 NLS 01 01 ENG V20100927 PDFAndy XiaoNessuna valutazione finora
- NTSE Stage 1 State Level Model Paper 14Documento4 pagineNTSE Stage 1 State Level Model Paper 14AmanNessuna valutazione finora
- Anatomy of A ClamDocumento6 pagineAnatomy of A ClamRU VickNessuna valutazione finora
- HeparinDocumento2 pagineHeparinNinoska Garcia-Ortiz100% (4)
- Template POMRDocumento8 pagineTemplate POMRPPDS IPD ULMNessuna valutazione finora
- Answer Key For Comprehensive Exam XVDocumento18 pagineAnswer Key For Comprehensive Exam XVQharts SajiranNessuna valutazione finora
- Fuel Metabolism in StarvationDocumento27 pagineFuel Metabolism in Starvationilluminel100% (2)
- Chronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsDocumento7 pagineChronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsAnonymous FgT04krgymNessuna valutazione finora
- Wound CareDocumento14 pagineWound CareKirsten Padilla Chua100% (4)
- Nervous System - All NotesDocumento6 pagineNervous System - All NotesJNessuna valutazione finora
- Neurotransmission, Measuring Chemical Events In: Advanced ArticleDocumento12 pagineNeurotransmission, Measuring Chemical Events In: Advanced ArticleazzaassNessuna valutazione finora
- Journal Reading Radiologi EllaDocumento44 pagineJournal Reading Radiologi EllaElla Putri SaptariNessuna valutazione finora
- Meridians and Points PDFDocumento35 pagineMeridians and Points PDFHamdon Hamad100% (9)
- Modul Anatomi Blok 7Documento27 pagineModul Anatomi Blok 7Dewandaru I A BNessuna valutazione finora
- H2S Training Slides ENGLISHDocumento46 pagineH2S Training Slides ENGLISHf.B100% (1)
- Vit CDocumento10 pagineVit C3/2 no.34 สรัญญากร สีหาราชNessuna valutazione finora