Potrebbero piacerti anche
- Dentine Hypersensitivity: Developing a Person-centred Approach to Oral HealthDa EverandDentine Hypersensitivity: Developing a Person-centred Approach to Oral HealthNessuna valutazione finora
- Dentin Hypersensitivity SeminarDocumento91 pagineDentin Hypersensitivity SeminarBharat Singh ChauhanNessuna valutazione finora
- Fixed Orthodontic Appliances: A Practical GuideDa EverandFixed Orthodontic Appliances: A Practical GuideValutazione: 1 su 5 stelle1/5 (1)
- Dentin HypersenstivityDocumento4 pagineDentin Hypersenstivitymohamed saadNessuna valutazione finora
- Oral Medicine & Pathology from A-ZDa EverandOral Medicine & Pathology from A-ZValutazione: 5 su 5 stelle5/5 (9)
- Dentin HypersensitivityDocumento44 pagineDentin Hypersensitivitytapobarna100% (1)
- Diagnostic Pulp TestingDocumento44 pagineDiagnostic Pulp TestingSree Harsha Gunneri100% (2)
- Case Presentation: Department of Oral Medicine, Diagnosis and RadiologyDocumento37 pagineCase Presentation: Department of Oral Medicine, Diagnosis and RadiologyDanzo VinsmokeNessuna valutazione finora
- Inflammation and Oral Cancer: From Bench to BedsideDa EverandInflammation and Oral Cancer: From Bench to BedsideHiroyuki TomitaNessuna valutazione finora
- Non-Surgical Periodontal Therapy Part 1 PDFDocumento106 pagineNon-Surgical Periodontal Therapy Part 1 PDFnsr_sweetyNessuna valutazione finora
- Perio Case HistoryDocumento90 paginePerio Case HistoryMoola Bharath ReddyNessuna valutazione finora
- Pit and Fissure SealantsDocumento34 paginePit and Fissure SealantsSamridhi SrivastavaNessuna valutazione finora
- The Prosthodontic Management of Endodontically Treated Teeth - A Literature Review. Part I. SuccesDocumento8 pagineThe Prosthodontic Management of Endodontically Treated Teeth - A Literature Review. Part I. SucceskochikaghochiNessuna valutazione finora
- Dentin Bonding Agents - An OverviewDocumento4 pagineDentin Bonding Agents - An OverviewIOSRjournalNessuna valutazione finora
- CementumDocumento10 pagineCementumAshish BisaneNessuna valutazione finora
- Dentinal HypersensitivityDocumento75 pagineDentinal HypersensitivityMica BernardoNessuna valutazione finora
- 2010 Textbook of Oral Medicine 2nd EditionDocumento1.179 pagine2010 Textbook of Oral Medicine 2nd EditionKeshav KantNessuna valutazione finora
- Avulsion SeminarDocumento54 pagineAvulsion Seminarrkc456Nessuna valutazione finora
- 08 - Salivary Biomarkers A Periodontal OverviewDocumento6 pagine08 - Salivary Biomarkers A Periodontal OverviewFisaNessuna valutazione finora
- Perio Case History 2Documento86 paginePerio Case History 2Moola Bharath Reddy100% (1)
- Antibiotics Used in DentistryDocumento17 pagineAntibiotics Used in Dentistrymegamarwa50% (2)
- EruptionDocumento18 pagineEruptionAnamika PandeyNessuna valutazione finora
- Imaging in Periodontics PerioDocumento49 pagineImaging in Periodontics PerioFourthMolar.comNessuna valutazione finora
- Diseases of Hard Tissues of Teeth PDFDocumento152 pagineDiseases of Hard Tissues of Teeth PDFAPARNA AARATHI SREEKUMARNessuna valutazione finora
- Dental CementsDocumento9 pagineDental CementscataNessuna valutazione finora
- Concepts of Enamel and Dentin AdhesionDocumento12 pagineConcepts of Enamel and Dentin Adhesionizeldien5870Nessuna valutazione finora
- Basic TxPlanning-Prognosis and Treatment Planning-Revised 9 September 2014Documento54 pagineBasic TxPlanning-Prognosis and Treatment Planning-Revised 9 September 2014DraspiNessuna valutazione finora
- Department of Oral & Maxillofacial Surgery: Rungta College of Dental Sciences & Research Kohka, BhilaiDocumento201 pagineDepartment of Oral & Maxillofacial Surgery: Rungta College of Dental Sciences & Research Kohka, BhilaiIrfan AliNessuna valutazione finora
- Aetiology of MalocclusionDocumento16 pagineAetiology of Malocclusionamen100% (2)
- List of Books and JournalsDocumento15 pagineList of Books and JournalsdentistdentistdentisNessuna valutazione finora
- Tests For Biocompatibility of Dental MaterialsDocumento151 pagineTests For Biocompatibility of Dental MaterialsDevanshi SharmaNessuna valutazione finora
- Dent Update 2016 Resin-Bonded-Bridge-DesignDocumento11 pagineDent Update 2016 Resin-Bonded-Bridge-DesignSmriti VermaNessuna valutazione finora
- Local Anesthesia Technique HandoutDocumento2 pagineLocal Anesthesia Technique Handoutmirfanulhaq100% (1)
- Dental PlaqueDocumento66 pagineDental PlaqueAnuj Singh PariharNessuna valutazione finora
- 1 Dental IndicesDocumento3 pagine1 Dental IndicesAinun Nur Arifah100% (2)
- Ankita Singh PG1 Year Department of Conservative Dentistry and EndodonticsDocumento94 pagineAnkita Singh PG1 Year Department of Conservative Dentistry and EndodonticssethupathiNessuna valutazione finora
- Impression Techniques For Management of Flabby Ridges in Complete DenturesDocumento6 pagineImpression Techniques For Management of Flabby Ridges in Complete DenturesDr Rohit Kumar Singh100% (1)
- Endo Perio LesionsDocumento24 pagineEndo Perio LesionsAneen Suresh0% (1)
- Tooth Development and Eruption c6Documento26 pagineTooth Development and Eruption c6Wy Gnoix100% (1)
- Stainless Steel CrownsDocumento24 pagineStainless Steel Crownswese87Nessuna valutazione finora
- Plaque ControlDocumento67 paginePlaque ControlAbdallah Essam Al-ZireeniNessuna valutazione finora
- Diseases of Periradicular TissuesDocumento62 pagineDiseases of Periradicular Tissuesanubhutigupta1404Nessuna valutazione finora
- Cracked Tooth SyndromeDocumento73 pagineCracked Tooth SyndromeShazeena OfficialNessuna valutazione finora
- The Periodontal Pocket PDFDocumento9 pagineThe Periodontal Pocket PDFIgnacio PulleyNessuna valutazione finora
- Management of Discoloured Teeth: Presented By: Amisha Jain M.D.S II YearDocumento44 pagineManagement of Discoloured Teeth: Presented By: Amisha Jain M.D.S II YearANUBHANessuna valutazione finora
- OHISDocumento11 pagineOHISKristina Robles100% (2)
- Dentogingival UnitDocumento53 pagineDentogingival Unitperiodontics0780% (5)
- Amalgam BondingDocumento21 pagineAmalgam BondingSaad Tanvir ShaikhNessuna valutazione finora
- Aggressive PeriodontitisDocumento101 pagineAggressive Periodontitisdileep900100% (1)
- Tooth Eruption and Its Disorders - Pediatric DentistryDocumento157 pagineTooth Eruption and Its Disorders - Pediatric DentistryPuneet ChoudharyNessuna valutazione finora
- NSAIDS in Dentistry It's Principles in PracticeDocumento6 pagineNSAIDS in Dentistry It's Principles in PracticeInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Development of TeethDocumento127 pagineDevelopment of Teethdentistpro.orgNessuna valutazione finora
- Trauma From Occlusion: Submitted by Saumya Bds 3rd Year 59Documento33 pagineTrauma From Occlusion: Submitted by Saumya Bds 3rd Year 59falakNessuna valutazione finora
- Dental Plaque: By:-Raina J. P. Khanam Post Graduate 2 Year Dept. of Periodontics and ImplantologyDocumento69 pagineDental Plaque: By:-Raina J. P. Khanam Post Graduate 2 Year Dept. of Periodontics and ImplantologyAtul KoundelNessuna valutazione finora
- Projection Geometry: Chhattisgarh Dental College & Research Institute, Sundra, Rajnandgaon (C.G.)Documento32 pagineProjection Geometry: Chhattisgarh Dental College & Research Institute, Sundra, Rajnandgaon (C.G.)vishal tiwary100% (2)
- Drug Interaction of Dental DrugsDocumento14 pagineDrug Interaction of Dental DrugsAnubhuti SabhlokNessuna valutazione finora
- Forces Acting On Restorations LD / Orthodontic Courses by Indian Dental AcademyDocumento95 pagineForces Acting On Restorations LD / Orthodontic Courses by Indian Dental Academyindian dental academyNessuna valutazione finora
- Antibiotics Use in DentistryDocumento5 pagineAntibiotics Use in DentistryIyad Abou-RabiiNessuna valutazione finora
- Criteria of SelectionDocumento12 pagineCriteria of SelectionVinisha Vipin SharmaNessuna valutazione finora
- Diff Betwn Inlay and Amalgam CavityDocumento7 pagineDiff Betwn Inlay and Amalgam CavityVinisha Vipin Sharma100% (1)
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDocumento6 pagineNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaNessuna valutazione finora
- Some Basics of LasersDocumento102 pagineSome Basics of LasersVinisha Vipin SharmaNessuna valutazione finora
- Challenges in Working Length DeterminationDocumento101 pagineChallenges in Working Length DeterminationVinisha Vipin SharmaNessuna valutazione finora
- Acupuncture in Dentistry PDFDocumento73 pagineAcupuncture in Dentistry PDFVinisha Vipin SharmaNessuna valutazione finora
- Mechanical Preparation Updated May2017 Prof Marco VersianiDocumento159 pagineMechanical Preparation Updated May2017 Prof Marco VersianiVinisha Vipin SharmaNessuna valutazione finora
- Laser in Conservative Dentistry & EndodonticsDocumento75 pagineLaser in Conservative Dentistry & EndodonticsVinisha Vipin SharmaNessuna valutazione finora
- Eaat 14 I 1 P 217Documento6 pagineEaat 14 I 1 P 217Vinisha Vipin SharmaNessuna valutazione finora
- Content ServerDocumento5 pagineContent ServerVinisha Vipin SharmaNessuna valutazione finora
- Content ServerDocumento6 pagineContent ServerVinisha Vipin SharmaNessuna valutazione finora
- Glide Path PreparationDocumento5 pagineGlide Path PreparationVinisha Vipin SharmaNessuna valutazione finora
- Show TextDocumento1 paginaShow TextVinisha Vipin SharmaNessuna valutazione finora
- EchsDocumento20 pagineEchsVinisha Vipin SharmaNessuna valutazione finora
- PRISMA-P Statement - Moher Sys Rev Jan 2015Documento9 paginePRISMA-P Statement - Moher Sys Rev Jan 2015Vinisha Vipin SharmaNessuna valutazione finora
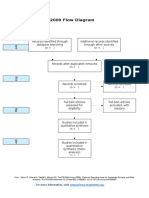
- PRISMA 2009 Flow Diagram: For More Information, VisitDocumento1 paginaPRISMA 2009 Flow Diagram: For More Information, VisitVinisha Vipin SharmaNessuna valutazione finora
- Practice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportDocumento5 paginePractice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportVinisha Vipin SharmaNessuna valutazione finora
- Ceramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveDocumento5 pagineCeramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveVinisha Vipin SharmaNessuna valutazione finora
- Esthetic Alternatives To AmalgamDocumento15 pagineEsthetic Alternatives To AmalgamVinisha Vipin SharmaNessuna valutazione finora
- Pin Retained RestorationDocumento31 paginePin Retained RestorationVinisha Vipin SharmaNessuna valutazione finora
- Clarks Cavity PreparationDocumento10 pagineClarks Cavity PreparationVinisha Vipin SharmaNessuna valutazione finora
- Nanodentistry: New Buzz in Dentistry: Review ArticleDocumento5 pagineNanodentistry: New Buzz in Dentistry: Review ArticleVinisha Vipin SharmaNessuna valutazione finora
- Management of Calcific Metamorphosis by Conventional Root Canal Treatment. A Case ReportDocumento5 pagineManagement of Calcific Metamorphosis by Conventional Root Canal Treatment. A Case ReportNguyễn Đức HoàngNessuna valutazione finora
- Cementum: Avisha AgrawalDocumento109 pagineCementum: Avisha AgrawalpoojaNessuna valutazione finora
- Pulp ProtactDocumento7 paginePulp ProtactFawaz AnwarNessuna valutazione finora
- DownloadDocumento250 pagineDownloadk8rbwkpgn7Nessuna valutazione finora
- Sturdevant's Art and Science of Operative Dentistry - South Asian EditionDocumento45 pagineSturdevant's Art and Science of Operative Dentistry - South Asian Editionsharon rajNessuna valutazione finora
- Oral and Dental HistologyDocumento6 pagineOral and Dental HistologyCésar HelenoNessuna valutazione finora
- Dentinal Hypersensitivity FinalDocumento99 pagineDentinal Hypersensitivity FinalSwijalNessuna valutazione finora
- CH 04Documento80 pagineCH 04flock_duxNessuna valutazione finora
- Enamel: Physical PropertiesDocumento18 pagineEnamel: Physical PropertiesRajat NangiaNessuna valutazione finora
- PULP - Oral Histo PDFDocumento5 paginePULP - Oral Histo PDFMaanNessuna valutazione finora
- Prometric Exam 2018Documento8 paginePrometric Exam 2018Sara Ben Amara100% (1)
- DentinDocumento12 pagineDentinsoumyadebsamanta2Nessuna valutazione finora
- Development and Growth of Teeth: Dr. Madhusudhan ReddyDocumento48 pagineDevelopment and Growth of Teeth: Dr. Madhusudhan ReddysiyaNessuna valutazione finora
- Cobourne (1999) The Genetic Control of Early OdontogenesisDocumento0 pagineCobourne (1999) The Genetic Control of Early OdontogenesisMaja Maja BułkaNessuna valutazione finora
- Regressive Alteration of TeethDocumento29 pagineRegressive Alteration of TeethLavanya Kalapala100% (3)
- MCQ 1060 QuestionsDocumento118 pagineMCQ 1060 Questionsapi-26291651100% (22)
- The Development of The TeethDocumento17 pagineThe Development of The TeethYasmin A. AhmedNessuna valutazione finora
- Stages of Tooth DevelopmentDocumento6 pagineStages of Tooth DevelopmentSOUMYA A DR, DEPT.OF DENTAL SCIENCES,SRIHERNessuna valutazione finora
- Biocompatibility of Dental MaterialsDocumento83 pagineBiocompatibility of Dental MaterialsSharique AlamNessuna valutazione finora
- The Effectiveness of Stem Cells Grafting On Regeneration of Dental Pulp: A Systematic Review and Meta-AnalysisDocumento11 pagineThe Effectiveness of Stem Cells Grafting On Regeneration of Dental Pulp: A Systematic Review and Meta-AnalysisIJAR JOURNALNessuna valutazione finora
- Endodontics Principles and Practice (001 138)Documento138 pagineEndodontics Principles and Practice (001 138)Daniel Ricardo Moreno HernandezNessuna valutazione finora
- Institute of Dentistry, CMH Lahore Medical College Curriculum & Study Guide First Year BDS Deaniod@cmhlahore - Edu.pkDocumento160 pagineInstitute of Dentistry, CMH Lahore Medical College Curriculum & Study Guide First Year BDS Deaniod@cmhlahore - Edu.pkSR Creations.Nessuna valutazione finora
- Anatomi Dan Fisiologi Mulut Bp2Documento47 pagineAnatomi Dan Fisiologi Mulut Bp2Aditya FirmansyahNessuna valutazione finora
- Low-Intensity Low-Frequency Ultrasound PromotesProliferation and Differentiation of Odontoblast-Like CellsDocumento6 pagineLow-Intensity Low-Frequency Ultrasound PromotesProliferation and Differentiation of Odontoblast-Like Cellsjuanesteban1890Nessuna valutazione finora
- Development of Dentition - FinalDocumento60 pagineDevelopment of Dentition - FinalDrkamesh M100% (1)
- Dental PulpDocumento53 pagineDental Pulpdr parveen bathla67% (3)
- Journal of Dentistry: Domenico Ricucci, Simona Loghin, Li-Na Niu, Franklin R. TayDocumento15 pagineJournal of Dentistry: Domenico Ricucci, Simona Loghin, Li-Na Niu, Franklin R. TayArturo Trejo VeraNessuna valutazione finora
- Preserving Pulp VitalityDocumento2 paginePreserving Pulp VitalitygsaveitNessuna valutazione finora
- MTA in The Treatment of Internal Root ResorptionDocumento6 pagineMTA in The Treatment of Internal Root ResorptionSaleh AlsadiNessuna valutazione finora
- Tugas Lapsus Dentine-Hypersensitivity-A-ReviewDocumento7 pagineTugas Lapsus Dentine-Hypersensitivity-A-ReviewSyifa MedikaNessuna valutazione finora