Potrebbero piacerti anche
- Testosterone Replacement Therapy, A Recipe For Success - John Crisler, D.O.Documento8 pagineTestosterone Replacement Therapy, A Recipe For Success - John Crisler, D.O.gstrohlNessuna valutazione finora
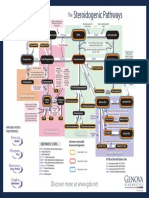
- The Steroidogenic PathwaysDocumento1 paginaThe Steroidogenic PathwaysMarkus van der WesthuizenNessuna valutazione finora
- ANS - Toxic Syndromes PDFDocumento74 pagineANS - Toxic Syndromes PDFARNessuna valutazione finora
- Diabetes Mellitus.Documento42 pagineDiabetes Mellitus.betablockers100% (1)
- Australian Diabetes Society Guidelines For Routine Glucose Control in HospitalDocumento70 pagineAustralian Diabetes Society Guidelines For Routine Glucose Control in HospitalYovan PrakosaNessuna valutazione finora
- Nephrotic Syndrome in Children: January 2013Documento7 pagineNephrotic Syndrome in Children: January 2013molenNessuna valutazione finora
- First Aid PsychiatryDocumento156 pagineFirst Aid PsychiatryMae Matira AbeladorNessuna valutazione finora
- Sketchy Pharm RuntimesDocumento6 pagineSketchy Pharm RuntimesRubayet Tasfin AlifNessuna valutazione finora
- Respiratory PharmacologyDocumento89 pagineRespiratory PharmacologyEka PuspitasariNessuna valutazione finora
- Rokh 2e ST4 PDFDocumento141 pagineRokh 2e ST4 PDFMahmud DipuNessuna valutazione finora
- Rheumatology Cases Fall Clinics 2019Documento85 pagineRheumatology Cases Fall Clinics 2019NaziBrola TsivadzeNessuna valutazione finora
- PPTDocumento61 paginePPTRheal P EsmailNessuna valutazione finora
- Differential Diagnosis of Valvular Heart DiseaseDocumento10 pagineDifferential Diagnosis of Valvular Heart DiseaseAbhisek ChatterjeeNessuna valutazione finora
- Biochemical Tests in Diabetes: DR Joe Fleming PHD MCB Frcpath Dept of Clinical Biochemistry CMC VelloreDocumento43 pagineBiochemical Tests in Diabetes: DR Joe Fleming PHD MCB Frcpath Dept of Clinical Biochemistry CMC Velloremariya khanNessuna valutazione finora
- Acid-Base Disorders NotesDocumento10 pagineAcid-Base Disorders NotesLovely100% (1)
- Endo Main Base LvivtechDocumento103 pagineEndo Main Base LvivtechGiridhar SolasaNessuna valutazione finora
- Practical Gastroenterology and Hepatology Board Review ToolkitDa EverandPractical Gastroenterology and Hepatology Board Review ToolkitKenneth R. DeVaultNessuna valutazione finora
- A Summary of The Chemical Mediators Involve in The Acute Inflammatory Response Is Shown in The Table BelowDocumento30 pagineA Summary of The Chemical Mediators Involve in The Acute Inflammatory Response Is Shown in The Table Belowinny100% (1)
- Pharmacology McqNEW 2Documento7 paginePharmacology McqNEW 2Ayman Ragab100% (2)
- 5 - Endocrinology Passmedicine Q. Bank PART I 2017Documento366 pagine5 - Endocrinology Passmedicine Q. Bank PART I 2017'محمد علي' محمد لافي100% (1)
- Drug Related ProblemsDocumento25 pagineDrug Related ProblemsChristine GanNessuna valutazione finora
- HemiplegiaDocumento11 pagineHemiplegiaFares EL DeenNessuna valutazione finora
- Metabolic Syndrome DR - Yunus, SPPDDocumento15 pagineMetabolic Syndrome DR - Yunus, SPPDMariaEllyNobetaHutabarat100% (1)
- WeitzmanDocumento5 pagineWeitzmandanielmoffatNessuna valutazione finora
- Acid Base Balance OR OR Regulation of Blood PHDocumento175 pagineAcid Base Balance OR OR Regulation of Blood PHhirendra patel100% (1)
- MRCP Paces DR Ahmed EliiwaDocumento3 pagineMRCP Paces DR Ahmed EliiwaGhulamMemonNessuna valutazione finora
- Alawlaqi - Obesity FinalDocumento26 pagineAlawlaqi - Obesity FinalMotea Alawlaqi100% (1)
- Rheumatoid Arthritis Final PDFDocumento47 pagineRheumatoid Arthritis Final PDFShirish kumarNessuna valutazione finora
- Question Bank For Mbbs Pediatrics: Long Essay - 20 MarksDocumento17 pagineQuestion Bank For Mbbs Pediatrics: Long Essay - 20 MarkspolluNessuna valutazione finora
- DiabeticcasestudyDocumento7 pagineDiabeticcasestudyapi-272773859Nessuna valutazione finora
- FC Derm (SA) Part II Past Papers - 2011 Mar 25-3-2014Documento4 pagineFC Derm (SA) Part II Past Papers - 2011 Mar 25-3-2014matentenNessuna valutazione finora
- Drug Dose Frank Shann 2017pdfDocumento173 pagineDrug Dose Frank Shann 2017pdfrezafahlevi31290Nessuna valutazione finora
- ConstipatiaDocumento34 pagineConstipatiaMaria Traian100% (2)
- 08&09 Oral Hypoglycemics-Level 11Documento48 pagine08&09 Oral Hypoglycemics-Level 11Usman Ali AkbarNessuna valutazione finora
- GP Reg - Asthma and Spirometry 2011Documento114 pagineGP Reg - Asthma and Spirometry 2011minerva_stanciuNessuna valutazione finora
- CVS II Tutorials Apr 12-17Documento7 pagineCVS II Tutorials Apr 12-17rishitNessuna valutazione finora
- Peptic Ulcer DiseaseDocumento22 paginePeptic Ulcer Diseaserosamundrae100% (1)
- Pud Case StudyDocumento8 paginePud Case Studyapi-346620455Nessuna valutazione finora
- Station 5 Cases 4Documento73 pagineStation 5 Cases 4Sagit Nauman81100% (1)
- Inborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Documento4 pagineInborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Wen Jie LauNessuna valutazione finora
- Renal PharmacologyDocumento52 pagineRenal Pharmacologyashraf0% (1)
- Physiology of DiabetesDocumento52 paginePhysiology of DiabetesPhysiology by Dr RaghuveerNessuna valutazione finora
- Nutritional AnemiaDocumento90 pagineNutritional AnemiaIrham KhairiNessuna valutazione finora
- Chemical Pathology II HIV AIDSDocumento33 pagineChemical Pathology II HIV AIDSSimeon AdebisiNessuna valutazione finora
- 4 - Endocrinology Tiki TakaDocumento32 pagine4 - Endocrinology Tiki TakaHemaNessuna valutazione finora
- 08 - Indications, Contraindications, Complications and Monitoring of enDocumento13 pagine08 - Indications, Contraindications, Complications and Monitoring of enbocah_britpopNessuna valutazione finora
- Magdy AbbasDocumento49 pagineMagdy AbbasAli AlisonNessuna valutazione finora
- 03 Cell InjuryDocumento72 pagine03 Cell InjuryLunaLure100% (1)
- Git 2Documento18 pagineGit 2Mateen ShukriNessuna valutazione finora
- Nephrology: Omar K MRCP IrelandDocumento54 pagineNephrology: Omar K MRCP IrelandManmeet SNessuna valutazione finora
- Guide To Revising SceDocumento6 pagineGuide To Revising Scepratim deyNessuna valutazione finora
- Pancytopenia 170119201048 PDFDocumento33 paginePancytopenia 170119201048 PDFDabogski France100% (1)
- Hyperlipidaemias (MRCP+ Step 1)Documento2 pagineHyperlipidaemias (MRCP+ Step 1)Yhr YhNessuna valutazione finora
- 2012 Complete Board Questions PDFDocumento43 pagine2012 Complete Board Questions PDFbmhshNessuna valutazione finora
- Psoriatic Arthritis UpdateDocumento42 paginePsoriatic Arthritis UpdateSudip MajumdarNessuna valutazione finora
- Rational Drug Prescribing Training CourseDocumento78 pagineRational Drug Prescribing Training CourseAhmadu Shehu MohammedNessuna valutazione finora
- Final Case Study PresentationDocumento49 pagineFinal Case Study Presentationapi-505518832Nessuna valutazione finora
- Medical InvestigationsDocumento7 pagineMedical InvestigationsmedpgnotesNessuna valutazione finora
- Motivation Letter MelfiDocumento2 pagineMotivation Letter Melfimelfip04Nessuna valutazione finora
- Hyperthyroidism: Prevalence Women 2% Men 0.2% 15% of Cases Occur in Patients Older Than 60 Years of AgeDocumento54 pagineHyperthyroidism: Prevalence Women 2% Men 0.2% 15% of Cases Occur in Patients Older Than 60 Years of AgeMegan MendozaNessuna valutazione finora
- Physiology Acid QuizDocumento5 paginePhysiology Acid QuizRavi AminNessuna valutazione finora
- Management of Diabetes Emergencies''Documento85 pagineManagement of Diabetes Emergencies''Princewill SeiyefaNessuna valutazione finora
- GERIATRIC MEDICINE (Basic)Documento41 pagineGERIATRIC MEDICINE (Basic)Medical AdvicesNessuna valutazione finora
- 11) ECG Pearls-Diagnosis You Don't Want To Miss - Dr. Noel ThomasDocumento104 pagine11) ECG Pearls-Diagnosis You Don't Want To Miss - Dr. Noel ThomasAbu Umayr100% (1)
- Fluid ResuscitationDocumento3 pagineFluid ResuscitationAdam FnsNessuna valutazione finora
- 2008 MCQDocumento6 pagine2008 MCQhelamahjoubmounirdmoNessuna valutazione finora
- Hypernatremia From HarrisonDocumento3 pagineHypernatremia From HarrisonNobel LaureateNessuna valutazione finora
- Hypoglycemia Treatment ProtocolDocumento1 paginaHypoglycemia Treatment ProtocolCherryBeeNessuna valutazione finora
- SOGP AnaemiaDocumento16 pagineSOGP AnaemiaMuhammad Farrukh ul IslamNessuna valutazione finora
- Nimovet: Nimesulide Injection 10% W/VDocumento1 paginaNimovet: Nimesulide Injection 10% W/VMano PraveenNessuna valutazione finora
- Drug Pricing Policy 2015 PDFDocumento21 pagineDrug Pricing Policy 2015 PDFSajidur Rehman SyedNessuna valutazione finora
- Formularium 2018 ADocumento213 pagineFormularium 2018 Asupril anshariNessuna valutazione finora
- USFDA - Pre-Approval InspectionDocumento53 pagineUSFDA - Pre-Approval Inspectionvg_vvgNessuna valutazione finora
- Morphine & PhenobarbitalDocumento6 pagineMorphine & PhenobarbitalfitriaNessuna valutazione finora
- Isman Firdaus, DR, SP - JP (K), FIHA: QualificationDocumento38 pagineIsman Firdaus, DR, SP - JP (K), FIHA: QualificationGhinna Septhiana PratiwiNessuna valutazione finora
- Vaccine Information For 11-Year-Old StudentsDocumento1 paginaVaccine Information For 11-Year-Old StudentsAnonymous gH0Y8V0Nessuna valutazione finora
- English For Nursing Topic 13 Explaining MedicationDocumento6 pagineEnglish For Nursing Topic 13 Explaining MedicationEha Huwaida HayatiNessuna valutazione finora
- Theophylline Use in Apnoea of Prematurity: Alison KerrDocumento27 pagineTheophylline Use in Apnoea of Prematurity: Alison KerrBhawna PandhuNessuna valutazione finora
- Untitled PresentationDocumento69 pagineUntitled PresentationWinary FitriaNessuna valutazione finora
- Deplin Patient BrochureDocumento16 pagineDeplin Patient BrochureAsif GhafoorNessuna valutazione finora
- Bps 1101 Drugs 101 2021: Wogilvie@uottawa - CaDocumento3 pagineBps 1101 Drugs 101 2021: Wogilvie@uottawa - Caritaelharti2012Nessuna valutazione finora
- Basics of Anaesthesia & NMBDocumento14 pagineBasics of Anaesthesia & NMBManish SinghNessuna valutazione finora
- FPM Amitriptyline PDFDocumento2 pagineFPM Amitriptyline PDFRheeza ElhaqNessuna valutazione finora
- Neuropharmacology: Danielle Larson, Tanya SimuniDocumento6 pagineNeuropharmacology: Danielle Larson, Tanya SimunigustavoNessuna valutazione finora
- Medical and Pharmacy Abbreviations (Sig Codes) : Abbreviation Meaning(s) CategoryDocumento3 pagineMedical and Pharmacy Abbreviations (Sig Codes) : Abbreviation Meaning(s) Categoryscope 3901Nessuna valutazione finora
- DS ClozapineDocumento3 pagineDS ClozapineMiggsNessuna valutazione finora
- DrugDocumento15 pagineDrugknxdg86vk2Nessuna valutazione finora
- Anti Anxiety DrugsDocumento26 pagineAnti Anxiety DrugsHamze Abdullah Al-ShawaheenNessuna valutazione finora
- Safety PharmacologyDocumento20 pagineSafety PharmacologyPranjal KothaleNessuna valutazione finora
- Subcutaneous Injection: Humalog U-100 or U-200: More CommonDocumento2 pagineSubcutaneous Injection: Humalog U-100 or U-200: More Commonahmad ryanNessuna valutazione finora