Potrebbero piacerti anche
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- PERITONITISDocumento67 paginePERITONITISSaraj DE Emperio100% (1)
- PERITONITISDocumento28 paginePERITONITISLily Yuri100% (1)
- PeritonitisDocumento11 paginePeritonitisMihir PatelNessuna valutazione finora
- Case of Obstructive JaundiceDocumento38 pagineCase of Obstructive JaundiceJay R Plogio100% (2)
- Cholelithiasis SneDocumento12 pagineCholelithiasis SneSuhas IngaleNessuna valutazione finora
- HerniaDocumento41 pagineHerniashobharamkrishna67% (3)
- Presented By:: Aamir Sharif HO at Hijaz HospitalDocumento27 paginePresented By:: Aamir Sharif HO at Hijaz HospitalnazmiNessuna valutazione finora
- CholelithiasisDocumento65 pagineCholelithiasisGAURAV0% (1)
- AppendicitisDocumento17 pagineAppendicitisAhmed Halaby100% (1)
- PeritonitisDocumento22 paginePeritonitisBobby Faisyal Rakhman100% (1)
- Renal AbscessDocumento13 pagineRenal Abscessawalsher100% (1)
- 21 Obstructive JaundiceDocumento12 pagine21 Obstructive JaundicejumaymayaNessuna valutazione finora
- Appendicitis PPT 1Documento30 pagineAppendicitis PPT 1Prashant Mishra100% (1)
- Intestinal Obstruction: Yohannes TDocumento34 pagineIntestinal Obstruction: Yohannes TVincent Ser100% (1)
- Acid Peptic DiseaseDocumento19 pagineAcid Peptic DiseaseKasuganti koteshwar rao100% (2)
- Urinary Tract InfectionDocumento50 pagineUrinary Tract Infectionpokhara gharipatanNessuna valutazione finora
- Cholelithiasis: Group MembersDocumento12 pagineCholelithiasis: Group MembersShiela GutierrezNessuna valutazione finora
- HEMATOCHEZIADocumento26 pagineHEMATOCHEZIAAlvin HartantoNessuna valutazione finora
- Obstructive JaundiceDocumento15 pagineObstructive JaundiceUjas Patel100% (4)
- Obstructive Jaundice: DR - Jamil SawakedDocumento62 pagineObstructive Jaundice: DR - Jamil SawakedAzizan HannyNessuna valutazione finora
- Cholelithiasis When They Are in The Bile CholedocolithiasisDocumento15 pagineCholelithiasis When They Are in The Bile Choledocolithiasishisabumohamed100% (1)
- Anorectal MalformationDocumento40 pagineAnorectal Malformationblessy83% (18)
- Chronic Liver DiseaseDocumento30 pagineChronic Liver Diseaseprajwal86% (7)
- Urinary Tract InfectionsDocumento53 pagineUrinary Tract InfectionsRapid Medicine100% (1)
- APPENDICITISDocumento36 pagineAPPENDICITISsjamilmdfauzie100% (4)
- Case HerniaDocumento42 pagineCase HerniaPurnamandala Abu FarisNessuna valutazione finora
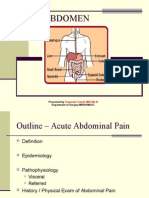
- Acute Abdominal PainDocumento72 pagineAcute Abdominal PainJoseph Stans Kasirye100% (1)
- CholelithiasisDocumento37 pagineCholelithiasisbaby padzNessuna valutazione finora
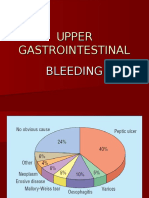
- Upper Gastrointestinal BleedingDocumento24 pagineUpper Gastrointestinal BleedingDr.Sathaporn Kunnathum100% (1)
- Acute Upper Airway Obstruction (Power Point)Documento21 pagineAcute Upper Airway Obstruction (Power Point)Sawsan Z. Jwaied100% (2)
- Peptic UlcerDocumento34 paginePeptic UlceralexjohnvtNessuna valutazione finora
- Liver AbscessDocumento15 pagineLiver AbscessAli Aborges Jr.Nessuna valutazione finora
- Phimosis and ParaphimosisDocumento9 paginePhimosis and ParaphimosisMuhammad Azzel Hanggara100% (3)
- Hypertrophic Pyloric StenosisDocumento17 pagineHypertrophic Pyloric StenosisMohammed Fareed100% (1)
- Intestinal Obstruction 4Documento25 pagineIntestinal Obstruction 4Muvenn KannanNessuna valutazione finora
- Anorectal MalformationsDocumento33 pagineAnorectal MalformationsVISS11Nessuna valutazione finora
- Urolithiasis SeminarDocumento50 pagineUrolithiasis SeminarSiddharth GuptaNessuna valutazione finora
- Bladder TraumaDocumento13 pagineBladder TraumaBernardNessuna valutazione finora
- Ascites: Pathogenesis and Clinical ApproachDocumento34 pagineAscites: Pathogenesis and Clinical ApproachPooja ShashidharanNessuna valutazione finora
- Intestinal Obstruction in Pediatric PatientsDocumento25 pagineIntestinal Obstruction in Pediatric PatientsHaryo Priambodo100% (1)
- Urolithiasis PowerpointDocumento41 pagineUrolithiasis PowerpointPinkrose Chiong FabellaNessuna valutazione finora
- GlomerulonephritisDocumento92 pagineGlomerulonephritisNita Hasan80% (5)
- CholecystitisDocumento34 pagineCholecystitisapi-26762768100% (1)
- Final EditDocumento43 pagineFinal EditMary Rose LinatocNessuna valutazione finora
- Fistula in AnoDocumento3 pagineFistula in Anokhadzx80% (5)
- Cholelithiasis: - Other Names: - Gallbladder Attack - Biliary Colic - Gallstone Attack - Bile Calculus - Biliary CalculusDocumento101 pagineCholelithiasis: - Other Names: - Gallbladder Attack - Biliary Colic - Gallstone Attack - Bile Calculus - Biliary CalculusYvonne100% (1)
- Cholecystitis and CholelithiasisDocumento19 pagineCholecystitis and CholelithiasisChristine Salimbagat100% (1)
- Upper Gi BleedingDocumento35 pagineUpper Gi Bleedingnawriirwan100% (1)
- Extrahepatic Biliary Tract Pathology - Cholidolithiasis, Cholidocholithiasis, Cholecystitis and CholangitisDocumento60 pagineExtrahepatic Biliary Tract Pathology - Cholidolithiasis, Cholidocholithiasis, Cholecystitis and CholangitisDarien LiewNessuna valutazione finora
- Intestinal Obstruction: MSU Medical Students. Batch 2. Group 2Documento31 pagineIntestinal Obstruction: MSU Medical Students. Batch 2. Group 2Qp Nizam100% (2)
- Liver AbscessDocumento19 pagineLiver AbscessAdi TrisnoNessuna valutazione finora
- HerniasDocumento64 pagineHerniasKalpana SubediNessuna valutazione finora
- PancreatitisDocumento7 paginePancreatitisavigenNessuna valutazione finora
- AchalasiaDocumento40 pagineAchalasiaedo andriyanto100% (1)
- Air Under DiaphragmDocumento16 pagineAir Under DiaphragmANSHU100% (1)
- Renal CalculiDocumento5 pagineRenal CalculiRufus Raj100% (1)
- Liver CancerDocumento44 pagineLiver CancerEjay Jacob Ricamara50% (2)
- KP 2.4.2.1 - PeritonitisDocumento27 pagineKP 2.4.2.1 - Peritonitisayuwulandari100% (1)
- Peritonitis: M. Iqbal RivaiDocumento27 paginePeritonitis: M. Iqbal RivaiFebri AnriyaniNessuna valutazione finora
- The Normal Tests: Preterm LaborDocumento3 pagineThe Normal Tests: Preterm LaborLily YuriNessuna valutazione finora
- Vaginal SeptumDocumento10 pagineVaginal SeptumLily YuriNessuna valutazione finora
- OmphaloceleDocumento8 pagineOmphaloceleLily YuriNessuna valutazione finora
- MasotongDocumento1 paginaMasotongLily YuriNessuna valutazione finora
- Victaulic-FP-FireLock Fire-Pac Series 745 PreactionDocumento9 pagineVictaulic-FP-FireLock Fire-Pac Series 745 PreactionTấn ĐạtNessuna valutazione finora
- Autodesk Design Review: About DWF and DWFXDocumento7 pagineAutodesk Design Review: About DWF and DWFXNesreNessuna valutazione finora
- Quizlet Table 7Documento1 paginaQuizlet Table 7JosielynNessuna valutazione finora
- Wind LoadingDocumento18 pagineWind LoadingStephen Ogalo100% (1)
- ProposalDocumento17 pagineProposalKhairul AkmalNessuna valutazione finora
- PLX Model OfficialDocumento105 paginePLX Model OfficialBảo Ngọc LêNessuna valutazione finora
- Components of Vectors Prepared By: Victor Rea OribeDocumento17 pagineComponents of Vectors Prepared By: Victor Rea OribeGerone Tolentino AtienzaNessuna valutazione finora
- Perfect Picture SummaryDocumento3 paginePerfect Picture SummaryReiaNessuna valutazione finora
- Theben Timer SUL 181DDocumento2 pagineTheben Timer SUL 181DFerdiNessuna valutazione finora
- DRUGPDocumento371 pagineDRUGPPolarogramaNessuna valutazione finora
- Lahainaluna High School Cafeteria: Lahaina, Maui, HawaiiDocumento42 pagineLahainaluna High School Cafeteria: Lahaina, Maui, HawaiiKeerthy MoniNessuna valutazione finora
- Game On Series BibleDocumento28 pagineGame On Series Bibleapi-513832615Nessuna valutazione finora
- PD750-01 Engine Data Sheet 12-29-20Documento4 paginePD750-01 Engine Data Sheet 12-29-20Service Brags & Hayes, Inc.Nessuna valutazione finora
- QLD Plan Draft Review Raw DataDocumento242 pagineQLD Plan Draft Review Raw DataRohit Jain100% (1)
- 28 ESL Discussion Topics Adult StudentsDocumento14 pagine28 ESL Discussion Topics Adult StudentsniallNessuna valutazione finora
- Advanced Packaging Polymers: Product Selection GuideDocumento12 pagineAdvanced Packaging Polymers: Product Selection GuideDKNessuna valutazione finora
- Glossary of Terms 2nd PartDocumento2 pagineGlossary of Terms 2nd Part2DJoyce D.N CapacieteNessuna valutazione finora
- Keira Knightley: Jump To Navigation Jump To SearchDocumento12 pagineKeira Knightley: Jump To Navigation Jump To SearchCrina LupuNessuna valutazione finora
- Panel Hospital List IGIDocumento6 paginePanel Hospital List IGIAbdul RahmanNessuna valutazione finora
- COSO DefinEDDocumento21 pagineCOSO DefinEDRefdy AnugrahNessuna valutazione finora
- Light Dimmer CircuitsDocumento14 pagineLight Dimmer CircuitskapilasriNessuna valutazione finora
- 2019q123.ev3-Descon Engro Level Gauges-QDocumento7 pagine2019q123.ev3-Descon Engro Level Gauges-Qengr_umer_01Nessuna valutazione finora
- Esp8285 Datasheet enDocumento29 pagineEsp8285 Datasheet enJohn GreenNessuna valutazione finora
- Appendicitis Case StudyDocumento6 pagineAppendicitis Case StudyKimxi Chiu LimNessuna valutazione finora
- Cell Structure, Cellular Respiration, PhotosynthesisDocumento14 pagineCell Structure, Cellular Respiration, PhotosynthesisAmr NasserNessuna valutazione finora
- Writing Short StoriesDocumento10 pagineWriting Short StoriesRodiatun YooNessuna valutazione finora
- Paper Format IJRDTDocumento3 paginePaper Format IJRDTrock starNessuna valutazione finora
- Q1. What Is JDBC? Explain Different Types JDBC Drivers With Suitable DiagramDocumento64 pagineQ1. What Is JDBC? Explain Different Types JDBC Drivers With Suitable DiagramjyebbwycqmfkuxNessuna valutazione finora
- Letter of Intent Date: 18-Feb-2019 Mr. Ravi Mishra,: For Multiplier Brand Solutions PVT LTDDocumento2 pagineLetter of Intent Date: 18-Feb-2019 Mr. Ravi Mishra,: For Multiplier Brand Solutions PVT LTDRavi MishraNessuna valutazione finora
- BZY Series Tension Meter ManualDocumento29 pagineBZY Series Tension Meter ManualJORGE SANTANDER0% (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDa EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisValutazione: 4 su 5 stelle4/5 (1)
- Breaking the Habit of Being YourselfDa EverandBreaking the Habit of Being YourselfValutazione: 4.5 su 5 stelle4.5/5 (1458)
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissDa EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissValutazione: 4.5 su 5 stelle4.5/5 (81)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipDa EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipValutazione: 4.5 su 5 stelle4.5/5 (1135)
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingDa EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingValutazione: 4.5 su 5 stelle4.5/5 (103)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDa EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningValutazione: 4 su 5 stelle4/5 (3)
- Love Yourself, Heal Your Life Workbook (Insight Guide)Da EverandLove Yourself, Heal Your Life Workbook (Insight Guide)Valutazione: 5 su 5 stelle5/5 (40)
- The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerDa EverandThe Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerValutazione: 4.5 su 5 stelle4.5/5 (58)
- The Creation Frequency: Tune In to the Power of the Universe to Manifest the Life of Your DreamsDa EverandThe Creation Frequency: Tune In to the Power of the Universe to Manifest the Life of Your DreamsValutazione: 5 su 5 stelle5/5 (549)
- Forever Strong: A New, Science-Based Strategy for Aging WellDa EverandForever Strong: A New, Science-Based Strategy for Aging WellNessuna valutazione finora
- Peaceful Sleep Hypnosis: Meditate & RelaxDa EverandPeaceful Sleep Hypnosis: Meditate & RelaxValutazione: 4.5 su 5 stelle4.5/5 (142)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayDa EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayNessuna valutazione finora
- Gut Health Hacks: 200 Ways to Balance Your Gut Microbiome and Improve Your Health!Da EverandGut Health Hacks: 200 Ways to Balance Your Gut Microbiome and Improve Your Health!Valutazione: 4.5 su 5 stelle4.5/5 (20)
- Strong Like Water: Finding the Freedom, Safety, and Compassion to Move through Hard Things--and Experience True FlourishingDa EverandStrong Like Water: Finding the Freedom, Safety, and Compassion to Move through Hard Things--and Experience True FlourishingValutazione: 4.5 su 5 stelle4.5/5 (33)
- Deep Sleep Hypnosis: Fall Asleep Instantly And Sleep WellDa EverandDeep Sleep Hypnosis: Fall Asleep Instantly And Sleep WellValutazione: 5 su 5 stelle5/5 (8)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouDa EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouValutazione: 3.5 su 5 stelle3.5/5 (5)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisDa EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisValutazione: 3 su 5 stelle3/5 (2)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeDa EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeValutazione: 3.5 su 5 stelle3.5/5 (13)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeDa EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNessuna valutazione finora
- Deep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!Da EverandDeep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!Valutazione: 4.5 su 5 stelle4.5/5 (10)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookDa EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookValutazione: 3.5 su 5 stelle3.5/5 (2)
- Really Very Crunchy: A Beginner's Guide to Removing Toxins from Your Life without Adding Them to Your PersonalityDa EverandReally Very Crunchy: A Beginner's Guide to Removing Toxins from Your Life without Adding Them to Your PersonalityValutazione: 5 su 5 stelle5/5 (28)
- Heal: Discover Your Unlimited Potential and Awaken the Powerful Healer WithinDa EverandHeal: Discover Your Unlimited Potential and Awaken the Powerful Healer WithinValutazione: 5 su 5 stelle5/5 (38)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyDa EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNessuna valutazione finora
- Eat & Run: My Unlikely Journey to Ultramarathon GreatnessDa EverandEat & Run: My Unlikely Journey to Ultramarathon GreatnessNessuna valutazione finora