Potrebbero piacerti anche
- Neonatal Jaundice CmeDocumento39 pagineNeonatal Jaundice CmeGideon K. Mutai100% (1)
- Neonatal Jaundice (Wong)Documento54 pagineNeonatal Jaundice (Wong)Siti Hajar100% (1)
- Neonatal Jaundice Lecture,,By DR Kassahun GirmaDocumento25 pagineNeonatal Jaundice Lecture,,By DR Kassahun GirmaKassahun Girma GelawNessuna valutazione finora
- Neonatal Jaundice CME ANisDocumento47 pagineNeonatal Jaundice CME ANisAnisNessuna valutazione finora
- JaundiceDocumento41 pagineJaundicesavina hasbianiNessuna valutazione finora
- Neo JaundiceDocumento67 pagineNeo Jaundicemanisha thakur100% (1)
- Neonatal JaundiceDocumento48 pagineNeonatal Jaundicelordoftheweb100% (22)
- OligohydramniosDocumento4 pagineOligohydramniossalamredNessuna valutazione finora
- Ectopic PregnancyDocumento26 pagineEctopic PregnancysandhyakrishnanNessuna valutazione finora
- Approach To Neonatal JaundiceDocumento73 pagineApproach To Neonatal JaundiceG Venkatesh50% (2)
- Neonatal HyperbilirubinemiaDocumento36 pagineNeonatal HyperbilirubinemiamahmmoudeltaweelNessuna valutazione finora
- Meconium Aspiration Syndrome (MAS)Documento12 pagineMeconium Aspiration Syndrome (MAS)Angela AmaoNessuna valutazione finora
- HyperbilirubinemiaDocumento10 pagineHyperbilirubinemiachiboogs456100% (1)
- CPDDocumento14 pagineCPDmaezuNessuna valutazione finora
- Neonatal HypoglycemiaDocumento22 pagineNeonatal HypoglycemiaRonak Sheth100% (3)
- ABO Incompatibility: By: Marvi Mae Jimena Rosean Marvi Joy M. YunsayDocumento14 pagineABO Incompatibility: By: Marvi Mae Jimena Rosean Marvi Joy M. Yunsaysagameteiro100% (1)
- Asphyxia NeonatorumDocumento34 pagineAsphyxia NeonatorumListya Paramita100% (1)
- Congenital Diaphragmatic HerniaDocumento21 pagineCongenital Diaphragmatic HerniaJennifer Dixon100% (1)
- Hypertension in Pregnancy: Margaret S. Hamilton, DNS, RNDocumento33 pagineHypertension in Pregnancy: Margaret S. Hamilton, DNS, RNHaji RajiNessuna valutazione finora
- HyperbilirubinemiaDocumento29 pagineHyperbilirubinemiaCham Ingalla Pascion88% (8)
- Neonatal Jaundice DrkumarDocumento44 pagineNeonatal Jaundice Drkumarvasu_5iveNessuna valutazione finora
- OB GDM CasepresDocumento102 pagineOB GDM Casepreskitten garciaNessuna valutazione finora
- Neonatal Jaundice: Dr. Nahed Al-NaggerDocumento25 pagineNeonatal Jaundice: Dr. Nahed Al-NaggerElok Pratiwi100% (2)
- Post-Partum HemorrhageDocumento15 paginePost-Partum Hemorrhageapi-257029163Nessuna valutazione finora
- Jaundice-Neonatal 2016Documento45 pagineJaundice-Neonatal 2016Awatef AbushhiwaNessuna valutazione finora
- Torch InfectionsDocumento27 pagineTorch InfectionsSimi SaiPrasoonNessuna valutazione finora
- Abhay Jain Roll No 126Documento20 pagineAbhay Jain Roll No 126abhay jainNessuna valutazione finora
- Ophthalmia NeonatorumDocumento19 pagineOphthalmia NeonatorumSanthu Tvm100% (1)
- Hyperbilirubinemia Case PresentationDocumento25 pagineHyperbilirubinemia Case PresentationEricka B. Banaszczuk100% (3)
- Perinatal Asphyxia - Outline of Pathophysiology and Recent Trends in ManagementDocumento31 paginePerinatal Asphyxia - Outline of Pathophysiology and Recent Trends in Managementokwadha simionNessuna valutazione finora
- Neonatal Hyperbilirubinemia and JaundiceDocumento8 pagineNeonatal Hyperbilirubinemia and JaundiceAndreea GeorgianaNessuna valutazione finora
- HIV in PregnancyDocumento28 pagineHIV in PregnancyRaja100% (1)
- Intrauterine Growth Restriction (IUGR)Documento7 pagineIntrauterine Growth Restriction (IUGR)redhoprayuda100% (1)
- Anemia in PregnancyDocumento17 pagineAnemia in Pregnancytharmasilen100% (1)
- High Risk NewbornDocumento21 pagineHigh Risk Newbornnaga maniNessuna valutazione finora
- Care of Neonate With HyperbilirubinemiaDocumento11 pagineCare of Neonate With HyperbilirubinemiaKakali ChakrabortyNessuna valutazione finora
- Congenital SyphilisDocumento6 pagineCongenital SyphilisFrozen Pandora MahayaNessuna valutazione finora
- Neonatal Hyperglycemia1Documento17 pagineNeonatal Hyperglycemia1Abhinav Mitra VatsNessuna valutazione finora
- Cord Presentation and ProlapseDocumento4 pagineCord Presentation and ProlapseAnnapurna Dangeti100% (2)
- Breech PresentationDocumento85 pagineBreech Presentationwidya vannesaNessuna valutazione finora
- Nursing Care of HyperbilirubinemiaDocumento12 pagineNursing Care of HyperbilirubinemiaFri-fri Manila67% (3)
- Meconium Aspiration SyndromeDocumento29 pagineMeconium Aspiration SyndromeAlwin Varghese T0% (1)
- Neonatal HyperbilirubinemiaDocumento22 pagineNeonatal Hyperbilirubinemiajoza29Nessuna valutazione finora
- Harika Priyanka. K Asst. Professor AconDocumento30 pagineHarika Priyanka. K Asst. Professor AconArchana MoreyNessuna valutazione finora
- GDMDocumento16 pagineGDMNorshahidah IedaNessuna valutazione finora
- Baby at Risk (NBU) NotesDocumento131 pagineBaby at Risk (NBU) NotesMercy KeruboNessuna valutazione finora
- Management of Neonatal JaundiceDocumento22 pagineManagement of Neonatal JaundiceSuhazeli Abdullah100% (1)
- Case Study On Meninomyocele (Repaired) PDocumento29 pagineCase Study On Meninomyocele (Repaired) Pcharanjit kaur100% (1)
- Neonatal JaundiceDocumento3 pagineNeonatal JaundicevorezNessuna valutazione finora
- Multiple PregnancyDocumento20 pagineMultiple PregnancyNurul Fahmiza TumiranNessuna valutazione finora
- Anorectal MalformationDocumento28 pagineAnorectal MalformationJaya Prabha50% (2)
- 27 Purpureal Venous Thrombosis and Pulmonary Embolism by Shambuling HebballiDocumento14 pagine27 Purpureal Venous Thrombosis and Pulmonary Embolism by Shambuling HebballiSamhitha Ayurvedic ChennaiNessuna valutazione finora
- Breech PresentationDocumento40 pagineBreech PresentationShuhada Wahab100% (3)
- Newborn AssessmentDocumento9 pagineNewborn Assessmentapi-237668254Nessuna valutazione finora
- Placenta Previa (New) - 1Documento32 paginePlacenta Previa (New) - 1Ibrahim ZainabNessuna valutazione finora
- Primary Uterine InertiaDocumento4 paginePrimary Uterine InertiaTrisha Cayabyab100% (1)
- Hemolytic Disease of The NewbornDocumento43 pagineHemolytic Disease of The Newbornalibayaty1Nessuna valutazione finora
- Icterus NeonatarumDocumento64 pagineIcterus NeonatarumDeepti KukretiNessuna valutazione finora
- Neonatal JaundiceDocumento45 pagineNeonatal JaundiceDrhassan HuseinNessuna valutazione finora
- Approach To Neonatal HyperbilirubinemiaDocumento34 pagineApproach To Neonatal HyperbilirubinemiaNilesh HatzadeNessuna valutazione finora
- Acute Leukaemia Presentation 1Documento20 pagineAcute Leukaemia Presentation 1Vaibhav KrishnaNessuna valutazione finora
- HIV in ChildrenDocumento11 pagineHIV in ChildrenVaibhav KrishnaNessuna valutazione finora
- History Taking in OrthopaedicsDocumento23 pagineHistory Taking in OrthopaedicsVaibhav Krishna100% (5)
- Manipal College of Medical Sciences Pokhara, Nepal: Erythema MultiformeDocumento56 pagineManipal College of Medical Sciences Pokhara, Nepal: Erythema MultiformeVaibhav KrishnaNessuna valutazione finora
- Approach To AnemiaDocumento33 pagineApproach To AnemiaVaibhav KrishnaNessuna valutazione finora
- Abdominal Pain in ChildrenDocumento15 pagineAbdominal Pain in ChildrenVaibhav KrishnaNessuna valutazione finora
- VSDDocumento29 pagineVSDVaibhav Krishna100% (2)
- Kernicterus: Sahisnuta BasnetDocumento10 pagineKernicterus: Sahisnuta BasnetVaibhav KrishnaNessuna valutazione finora
- Schizophrenia: Disturbances Thinking in Feeling BehaviorDocumento26 pagineSchizophrenia: Disturbances Thinking in Feeling BehaviorVaibhav KrishnaNessuna valutazione finora
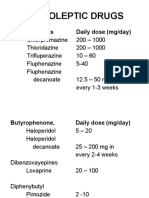
- Neuroleptic Drugs: Phenothiazines Daily Dose (Mg/day)Documento11 pagineNeuroleptic Drugs: Phenothiazines Daily Dose (Mg/day)Vaibhav KrishnaNessuna valutazione finora
- Antidepressants: I. Cyclic AntidepressantDocumento17 pagineAntidepressants: I. Cyclic AntidepressantVaibhav KrishnaNessuna valutazione finora
- Shoulder DystociaDocumento38 pagineShoulder DystociaVaibhav Krishna100% (1)
- Dissociation DisorderDocumento33 pagineDissociation DisorderVaibhav KrishnaNessuna valutazione finora
- Thyroid StormDocumento33 pagineThyroid StormVaibhav Krishna50% (2)
- Anxiety DisorderDocumento26 pagineAnxiety DisorderVaibhav KrishnaNessuna valutazione finora
- 3rd Stage of LabourDocumento16 pagine3rd Stage of LabourVaibhav KrishnaNessuna valutazione finora
- Curriculum Vitae: Name: Yousif Mohamed Yousif Abdallah Birth Date: Nationality: M. Status: Language: E. MailDocumento17 pagineCurriculum Vitae: Name: Yousif Mohamed Yousif Abdallah Birth Date: Nationality: M. Status: Language: E. MailHassan NileNessuna valutazione finora
- Susan-Michie-slides Nov 12 2015 PDFDocumento63 pagineSusan-Michie-slides Nov 12 2015 PDFPankajNessuna valutazione finora
- AsthmaDocumento39 pagineAsthmamits98Nessuna valutazione finora
- Acute Leukemia: Basic PrinciplesDocumento3 pagineAcute Leukemia: Basic PrinciplesPrabhat GuptaNessuna valutazione finora
- The Medicinal PlantsDocumento42 pagineThe Medicinal PlantsEclud100% (3)
- Garcinia Kola ThesisDocumento36 pagineGarcinia Kola ThesisDdn RmaNessuna valutazione finora
- AmputationDocumento160 pagineAmputationChamalla Deepak100% (4)
- Typhoid Fever Case StudyDocumento18 pagineTyphoid Fever Case Studyiurae50% (2)
- Airway Management - DR Dedi SpAnDocumento120 pagineAirway Management - DR Dedi SpAnBagus Abdillah WinataNessuna valutazione finora
- Genetic and Biological Hallmarks of Colorectal CancerDocumento34 pagineGenetic and Biological Hallmarks of Colorectal CancerFredNessuna valutazione finora
- Kidney CancerDocumento31 pagineKidney CancerEfren Elico VenguaNessuna valutazione finora
- DM OAD 14 - RevDocumento36 pagineDM OAD 14 - RevAri AsriniNessuna valutazione finora
- Differentiated Thyroid Cancer: How Do Current Practice Guidelines Affect Management?Documento8 pagineDifferentiated Thyroid Cancer: How Do Current Practice Guidelines Affect Management?wafasahilahNessuna valutazione finora
- Ovarian Cyst: ClassificationDocumento31 pagineOvarian Cyst: ClassificationZozo Shadap100% (2)
- Goljan Errata SheetDocumento11 pagineGoljan Errata SheetVishala MishraNessuna valutazione finora
- Khul Gariin TseguudDocumento7 pagineKhul Gariin TseguudMaggi BoldNessuna valutazione finora
- CA EndometriumDocumento46 pagineCA EndometriumNovianaHartikasariNessuna valutazione finora
- MSDS - Indikator PPDocumento7 pagineMSDS - Indikator PPPertamax MahoNessuna valutazione finora
- Radicular SyndromeDocumento40 pagineRadicular Syndromeainulhawa89Nessuna valutazione finora
- Contemporary Evaluation and Management of Parathyroid CarcinomaDocumento6 pagineContemporary Evaluation and Management of Parathyroid CarcinomaIvanna JaramilloNessuna valutazione finora
- Department of Bio-Informatics 3 Semester (Morning) : Subject ImmunologyDocumento10 pagineDepartment of Bio-Informatics 3 Semester (Morning) : Subject ImmunologyShaher Bano MirzaNessuna valutazione finora
- 7 Bali Cardiology Update 2018Documento14 pagine7 Bali Cardiology Update 2018nova cintyaNessuna valutazione finora
- Pemeriksaan Colok DuburDocumento9 paginePemeriksaan Colok DuburRidwan Hadinata SalimNessuna valutazione finora
- Total Glossectomy For Tongue CancerDocumento10 pagineTotal Glossectomy For Tongue CancerRajan KarmakarNessuna valutazione finora
- Med Surg 2 - 10 Nursing Care of Clients With Biliary DisordersDocumento4 pagineMed Surg 2 - 10 Nursing Care of Clients With Biliary DisordersMaxinne RoseñoNessuna valutazione finora
- ALZHEIMERDocumento9 pagineALZHEIMERKhem Limoso100% (2)
- Creatine Kinase. by AsifDocumento10 pagineCreatine Kinase. by AsifharisNessuna valutazione finora
- DRUG NAME: Rituximab: Synonym (S) : Common Trade Name (S) : ClassificationDocumento12 pagineDRUG NAME: Rituximab: Synonym (S) : Common Trade Name (S) : ClassificationpmuftiaNessuna valutazione finora
- Ijvm June 2011 FinalDocumento64 pagineIjvm June 2011 FinalAmitesh DubeyNessuna valutazione finora