Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Show Us Your Talents 96019Documento1 paginaShow Us Your Talents 96019Kadek DharmawanNessuna valutazione finora
- Traditional CostumeDocumento8 pagineTraditional CostumeKadek DharmawanNessuna valutazione finora
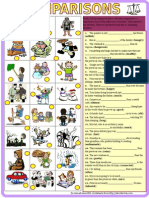
- 8028 Comparisons Comparative Superlative With KeyDocumento2 pagine8028 Comparisons Comparative Superlative With KeyGoldFrosch40% (5)
- Animal Body Parts 17053Documento1 paginaAnimal Body Parts 17053Kadek DharmawanNessuna valutazione finora
- What Do You Know About Jobs - 28056Documento2 pagineWhat Do You Know About Jobs - 28056Kadek DharmawanNessuna valutazione finora
- Expert Judgment Sheet For: - Judge: - No Expert Response Suggestion Relevant IrrelevantDocumento1 paginaExpert Judgment Sheet For: - Judge: - No Expert Response Suggestion Relevant IrrelevantKadek DharmawanNessuna valutazione finora
- Uji ValiditasDocumento2 pagineUji ValiditasKadek DharmawanNessuna valutazione finora
- DafsusDocumento1 paginaDafsusKadek DharmawanNessuna valutazione finora
- Tonsilitis 2Documento8 pagineTonsilitis 2Kadek DharmawanNessuna valutazione finora
- Uji ValiditasDocumento2 pagineUji ValiditasKadek DharmawanNessuna valutazione finora
- DR Amin Aging and CellsDocumento23 pagineDR Amin Aging and CellsSriwiie NarniNessuna valutazione finora
- DafsusDocumento1 paginaDafsusKadek DharmawanNessuna valutazione finora
- Aging Process in The EyeDocumento68 pagineAging Process in The EyeKadek DharmawanNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Chapter 18 Metric and Imperial Measures: Scheme of WorkDocumento2 pagineChapter 18 Metric and Imperial Measures: Scheme of WorkrightwayNessuna valutazione finora
- 2 BA British and American Life and InstitutionsDocumento3 pagine2 BA British and American Life and Institutionsguest1957Nessuna valutazione finora
- Baywatch - Tower of PowerDocumento20 pagineBaywatch - Tower of Powerkazimkoroglu@hotmail.comNessuna valutazione finora
- Perfumery in Ancient IndiaDocumento9 paginePerfumery in Ancient IndiaRachel ChittilapillyNessuna valutazione finora
- CibaDocumento16 pagineCibamaheshgupte0% (1)
- Science Revision Sheet Year 7 Periodic 2Documento5 pagineScience Revision Sheet Year 7 Periodic 2malknabih699Nessuna valutazione finora
- PMO Crossword 1Documento4 paginePMO Crossword 1Waseem NosimohomedNessuna valutazione finora
- Wed 0945-Avionics Modernization For LegacyDocumento38 pagineWed 0945-Avionics Modernization For LegacygasparferrerNessuna valutazione finora
- GSPL Annual ReportDocumento190 pagineGSPL Annual Reportjai chaudhariNessuna valutazione finora
- The Oxford Handbook of The Trinity (Introducción)Documento12 pagineThe Oxford Handbook of The Trinity (Introducción)casandraentroya100% (1)
- CV TemplateDocumento4 pagineCV TemplateIri PopescuNessuna valutazione finora
- Toefl Exercise 1Documento9 pagineToefl Exercise 1metaNessuna valutazione finora
- The Ambiguity of Micro-UtopiasDocumento8 pagineThe Ambiguity of Micro-UtopiaspolkleNessuna valutazione finora
- State Bank of India: Re Cruitme NT of Clerical StaffDocumento3 pagineState Bank of India: Re Cruitme NT of Clerical StaffthulasiramaswamyNessuna valutazione finora
- Writing Kafani or AlfiDocumento5 pagineWriting Kafani or AlfisahebjuNessuna valutazione finora
- Programme Guide - PGDMCH PDFDocumento58 pagineProgramme Guide - PGDMCH PDFNJMU 2006Nessuna valutazione finora
- Orange PeelDocumento2 pagineOrange PeelCharul Shukla100% (1)
- Canada's Top 50 FinTech CompaniesDocumento16 pagineCanada's Top 50 FinTech CompaniesTina SmithNessuna valutazione finora
- 2016 May Virginia Medical Law ReportDocumento20 pagine2016 May Virginia Medical Law ReportMichael DuntzNessuna valutazione finora
- Rheumatoid ArthritisDocumento15 pagineRheumatoid ArthritisPJHG100% (2)
- Dengue Syndrome: Presented By: A.Sahaya Mary M.SC Nursing I Yr Scon, SimatsDocumento57 pagineDengue Syndrome: Presented By: A.Sahaya Mary M.SC Nursing I Yr Scon, Simatssagi muNessuna valutazione finora
- Essentials or Legal Rules As To ProposalDocumento7 pagineEssentials or Legal Rules As To ProposalmasoodNessuna valutazione finora
- Hamlet Greek TragedyDocumento21 pagineHamlet Greek TragedyJorge CanoNessuna valutazione finora
- The Writing Life by Annie DillardDocumento60 pagineThe Writing Life by Annie DillardkishorsandageNessuna valutazione finora
- Map of Jeju: For Muslim TouristsDocumento7 pagineMap of Jeju: For Muslim TouristslukmannyeoNessuna valutazione finora
- Erinnerungsmotive in Wagner's Der Ring Des NibelungenDocumento14 pagineErinnerungsmotive in Wagner's Der Ring Des NibelungenLaur MatysNessuna valutazione finora
- Global Value Chain: Shikha GuptaDocumento19 pagineGlobal Value Chain: Shikha GuptaRushilNessuna valutazione finora
- Dauns Prime Module 1978Documento26 pagineDauns Prime Module 1978Ivan AdrianNessuna valutazione finora
- Holly Rayner - The Prince S Real Fake BrideDocumento239 pagineHolly Rayner - The Prince S Real Fake BrideAbbyMac BNessuna valutazione finora
- Kapil Choudhary: Personal ProfileDocumento2 pagineKapil Choudhary: Personal ProfileAishwarya GoelNessuna valutazione finora