Potrebbero piacerti anche
- Bronchial AsthmaDocumento46 pagineBronchial AsthmaKhor Kee GuanNessuna valutazione finora
- CPC Acute AppendicitisDocumento57 pagineCPC Acute AppendicitisYS Nate100% (1)
- Cor Pulmonale PresentationDocumento17 pagineCor Pulmonale Presentationandi reskifaisNessuna valutazione finora
- GP Reg - Asthma and Spirometry 2011Documento114 pagineGP Reg - Asthma and Spirometry 2011minerva_stanciuNessuna valutazione finora
- Hyperthyroidism History TakingDocumento11 pagineHyperthyroidism History TakingmokkailinNessuna valutazione finora
- ShockDocumento21 pagineShockNyakie MotlalaneNessuna valutazione finora
- Name: Wong Wai Kheong Matrix No: BMS12081154Documento13 pagineName: Wong Wai Kheong Matrix No: BMS12081154myolie wuNessuna valutazione finora
- Abdominal Swelling + AscitesDocumento29 pagineAbdominal Swelling + AscitesDevina CiayadiNessuna valutazione finora
- Seminar 2 (Paeds)Documento31 pagineSeminar 2 (Paeds)Jonathan YeohNessuna valutazione finora
- Bronchial AsthmaDocumento21 pagineBronchial AsthmashaitabliganNessuna valutazione finora
- Bronchial AsthmaDocumento54 pagineBronchial AsthmaSehar162100% (2)
- Acute Respiratory Distress SyndromDocumento38 pagineAcute Respiratory Distress SyndrompatriaindraNessuna valutazione finora
- History Taking Cheat SheetDocumento1 paginaHistory Taking Cheat SheetLaura ForsythNessuna valutazione finora
- Guide To Assessment and Management of Acute Gastroenteritis in Primary CareDocumento2 pagineGuide To Assessment and Management of Acute Gastroenteritis in Primary CareMaya LarasNessuna valutazione finora
- AsthmaDocumento39 pagineAsthmamits98Nessuna valutazione finora
- Notes On History Taking in The Cardiovascular SystemDocumento10 pagineNotes On History Taking in The Cardiovascular Systemmdjohar72Nessuna valutazione finora
- Lower Respiratory Tract InfectionDocumento9 pagineLower Respiratory Tract InfectionNamrah AfzalNessuna valutazione finora
- Bronchial AsthmaDocumento39 pagineBronchial AsthmaSaeed mohamed100% (1)
- History Taking of Respiratory SystemDocumento24 pagineHistory Taking of Respiratory SystemNadiya Elfira BilqisNessuna valutazione finora
- Derma Case Write UpDocumento9 pagineDerma Case Write UpAmbhi GanaNessuna valutazione finora
- Case PresentationDocumento20 pagineCase PresentationMohamad HafyfyNessuna valutazione finora
- Poisoning in ChildrenDocumento11 paginePoisoning in ChildrenAndriana HalfienNessuna valutazione finora
- Case AppendicitisDocumento30 pagineCase AppendicitisSarahNessuna valutazione finora
- Bronchial AsthmaDocumento71 pagineBronchial AsthmaHero MondaresNessuna valutazione finora
- Approach To A Child With Cough and Difficulty in BreathingDocumento23 pagineApproach To A Child With Cough and Difficulty in BreathingKashif Burki100% (2)
- Chest InjuriesDocumento19 pagineChest InjuriesAbdi Kumala100% (1)
- Final GIT Case PresentationDocumento53 pagineFinal GIT Case PresentationRovan100% (1)
- Congestive Cardiac Failure by NeetaDocumento26 pagineCongestive Cardiac Failure by NeetaNeeta AnandaNessuna valutazione finora
- Pyogenic MeningitisDocumento46 paginePyogenic MeningitisShahnaaz ShahNessuna valutazione finora
- Reye's SyndromeDocumento11 pagineReye's SyndromeChristine Go100% (1)
- Acute Bronchiolitis EditedDocumento19 pagineAcute Bronchiolitis EditedSurgicalgownNessuna valutazione finora
- Acute Poisoning of Therapeutic Agents: by Alemayehu TomaDocumento42 pagineAcute Poisoning of Therapeutic Agents: by Alemayehu TomaYohannis AsefaNessuna valutazione finora
- Different Types of AsthmaDocumento16 pagineDifferent Types of AsthmaAmira Saidin0% (1)
- Approach To Fever and AntibioticsDocumento13 pagineApproach To Fever and Antibioticsasraf amirullahNessuna valutazione finora
- The Pneumonias: Associate Professor Dr. Lauren Ţiu ŞorodocDocumento60 pagineThe Pneumonias: Associate Professor Dr. Lauren Ţiu ŞorodocCristina Georgiana CoticăNessuna valutazione finora
- CASE 2 PneumoniaDocumento12 pagineCASE 2 PneumoniaKenneth MiguelNessuna valutazione finora
- AKI CASE NishaDocumento64 pagineAKI CASE NishaSurkhali Bipana100% (1)
- Laproscopic SurgeryDocumento80 pagineLaproscopic SurgeryAqeel AhmadNessuna valutazione finora
- Asthma Management and Prevention in ChildrenDocumento57 pagineAsthma Management and Prevention in ChildrenSundararajaperumal AnandhakrishnanNessuna valutazione finora
- Gestational DiabetesDocumento37 pagineGestational DiabetesSm BadruddozaNessuna valutazione finora
- Bronchial Asthma (I, II &III) LecturesDocumento102 pagineBronchial Asthma (I, II &III) Lecturesibnbasheer100% (5)
- Dental Abscess - Symptoms, Diagnosis and Treatment - BMJ Best PracticeDocumento1 paginaDental Abscess - Symptoms, Diagnosis and Treatment - BMJ Best PracticeTri Sakti Sunda RomdhoniNessuna valutazione finora
- Problem-based Approach to Gastroenterology and HepatologyDa EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNessuna valutazione finora
- By: DR Eyad Talal: Moderator: DR I - QudaisatDocumento55 pagineBy: DR Eyad Talal: Moderator: DR I - QudaisatEyad AbdeljawadNessuna valutazione finora
- Chronic Suppurative Otitis MediaDocumento11 pagineChronic Suppurative Otitis MediaaditiarrtuguNessuna valutazione finora
- Common Histories and Red Flags Presentation Noninteractive VersionDocumento21 pagineCommon Histories and Red Flags Presentation Noninteractive VersionesmarNessuna valutazione finora
- Copd 200412082048Documento139 pagineCopd 200412082048Richard ArceNessuna valutazione finora
- Problems in Early PregnancyDocumento11 pagineProblems in Early PregnancyRizal LeonardoNessuna valutazione finora
- Broncho Pneumonia CaseDocumento52 pagineBroncho Pneumonia CaseprsentNessuna valutazione finora
- Approach To The Surgical PatientDocumento51 pagineApproach To The Surgical Patientsanjivdas100% (1)
- An Approach To A Patient With BreathlessnessDocumento35 pagineAn Approach To A Patient With Breathlessnessgl tousifNessuna valutazione finora
- Cerebral Malaria (CM) Prof. WBP Matuja, MuhasDocumento20 pagineCerebral Malaria (CM) Prof. WBP Matuja, MuhasAnonymous TCZf45C10Nessuna valutazione finora
- Bronchiolitis in ChildrenDocumento16 pagineBronchiolitis in ChildrenNym Angga Santosa100% (1)
- Chest Pain Non TraumaDocumento45 pagineChest Pain Non TraumaTita LuthfiaNessuna valutazione finora
- Shock, Sirs & ModsDocumento37 pagineShock, Sirs & ModsambitioustamannaNessuna valutazione finora
- Anaest CWU ICUDocumento13 pagineAnaest CWU ICUHana FauziNessuna valutazione finora
- Dengue Fever in Pregnancy 2Documento37 pagineDengue Fever in Pregnancy 2Kevin AgbonesNessuna valutazione finora
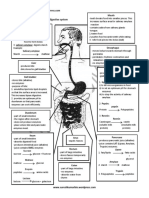
- Human Digestive PDFDocumento1 paginaHuman Digestive PDFsiyin limNessuna valutazione finora
- Fundamental Types of NeuronsDocumento28 pagineFundamental Types of NeuronsShidevNessuna valutazione finora
- Modul Matematik Tingkatan 4Documento9 pagineModul Matematik Tingkatan 4Nur Nadiah100% (1)
- Clinical EnzymologyDocumento14 pagineClinical EnzymologyShidevNessuna valutazione finora
- PH Le BotomyDocumento114 paginePH Le Botomynidal_Daqa100% (2)
- Vision 1Documento22 pagineVision 1ShidevNessuna valutazione finora
- Time Test 1 Multiple Choice Questions: Name: ID: CohortDocumento3 pagineTime Test 1 Multiple Choice Questions: Name: ID: CohortShidevNessuna valutazione finora
- As BiologyDocumento127 pagineAs BiologyRob Gomez100% (5)
- Motion With Uniform AccelerationDocumento3 pagineMotion With Uniform AccelerationShidevNessuna valutazione finora
- 2.10 Work, Power, and EfficiencyDocumento20 pagine2.10 Work, Power, and EfficiencyShidevNessuna valutazione finora
- Mid Year Exam (May 2017) Exam Scope: Form 4 (Chapter 1 Till 3)Documento1 paginaMid Year Exam (May 2017) Exam Scope: Form 4 (Chapter 1 Till 3)ShidevNessuna valutazione finora
- Neuron TeacherDocumento1 paginaNeuron TeacherShidevNessuna valutazione finora
- SPM Physics Formula List Form5Documento18 pagineSPM Physics Formula List Form5ShidevNessuna valutazione finora
- Physics Short Notes Form 4Documento16 paginePhysics Short Notes Form 4Amni Aliasak86% (44)
- Motion With Uniform AccelerationDocumento3 pagineMotion With Uniform AccelerationShidevNessuna valutazione finora
- Science f5Documento7 pagineScience f5Dinesh CidocNessuna valutazione finora
- Tips Physics SPMDocumento25 pagineTips Physics SPMShidevNessuna valutazione finora
- Sunway A Level Math Logic Challenge 2010Documento9 pagineSunway A Level Math Logic Challenge 2010Faith HoNessuna valutazione finora
- Sunway A Level Math Logic Challenge 2010Documento9 pagineSunway A Level Math Logic Challenge 2010Faith HoNessuna valutazione finora
- Movement With Uniform Acceleration: Answering Exam QuestionsDocumento2 pagineMovement With Uniform Acceleration: Answering Exam QuestionsChristopher AuNessuna valutazione finora
- Vts3gimifexy U GXRBDocumento1 paginaVts3gimifexy U GXRBShidevNessuna valutazione finora
- Form 4 Physics ExercisesDocumento10 pagineForm 4 Physics ExercisesShidevNessuna valutazione finora
- Module DuaDocumento8 pagineModule DuaNisa Hj MohamadNessuna valutazione finora
- A Addition Operation or Subtraction OperationDocumento1 paginaA Addition Operation or Subtraction OperationShidevNessuna valutazione finora
- Prostae UroDocumento43 pagineProstae UroShidevNessuna valutazione finora
- Sunway A Level Math Logic Challenge 2010Documento9 pagineSunway A Level Math Logic Challenge 2010Faith HoNessuna valutazione finora
- F4 ExperimentsDocumento52 pagineF4 ExperimentsKiTTy94% (16)
- 2.8 GravityDocumento26 pagine2.8 GravityShidevNessuna valutazione finora
- Topic 4 PowerDocumento8 pagineTopic 4 PowerShidevNessuna valutazione finora
- Topic 1Documento7 pagineTopic 1ShidevNessuna valutazione finora
- Clinical Cases Mrcpch1Documento223 pagineClinical Cases Mrcpch1aeyousef100% (1)
- Drug Study FormatDocumento20 pagineDrug Study FormatTrisha SuazoNessuna valutazione finora
- Salbu IpaDocumento2 pagineSalbu IpaGwyn RosalesNessuna valutazione finora
- AntitussivesDocumento5 pagineAntitussivesAditya PrajapatiNessuna valutazione finora
- Topic 2 COPD and AsthmaDocumento18 pagineTopic 2 COPD and AsthmaCaitlynNessuna valutazione finora
- Pharmacology of SalbutamolDocumento11 paginePharmacology of SalbutamolarvinthamelakaNessuna valutazione finora
- Aerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatec Rinovagos, Atrovent, Atrovent HFADocumento3 pagineAerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatec Rinovagos, Atrovent, Atrovent HFAGwyn RosalesNessuna valutazione finora
- Anatomy and Physiology CopdDocumento15 pagineAnatomy and Physiology CopdAssenav May100% (3)
- Final Med WardDocumento30 pagineFinal Med WardNasrima D. MacarayaNessuna valutazione finora
- LIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyDocumento19 pagineLIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyBenjamin TantiansuNessuna valutazione finora
- Drug Study Copd FinalDocumento3 pagineDrug Study Copd FinalMaverick LimNessuna valutazione finora
- Pud Drug StudyDocumento6 paginePud Drug StudyLolcoma15 JaymsNessuna valutazione finora
- 2 Cholinergic BlockersDocumento49 pagine2 Cholinergic BlockersAmanuel MaruNessuna valutazione finora
- Broncho DilatorsDocumento53 pagineBroncho DilatorsDocRNNessuna valutazione finora
- Drugs in Treatment of Bronchial AsthmaDocumento46 pagineDrugs in Treatment of Bronchial AsthmaNikita JangraNessuna valutazione finora
- Drug Study PediaDocumento5 pagineDrug Study Pediajulesubayubay5428Nessuna valutazione finora
- BAIAE'Patient's IllnessDocumento10 pagineBAIAE'Patient's Illnessq_t_jheng1603Nessuna valutazione finora
- Metered Dose InhalersDocumento2 pagineMetered Dose InhalersTepperoniNessuna valutazione finora
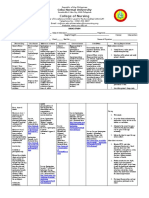
- College of Nursing: Cebu Normal UniversityDocumento4 pagineCollege of Nursing: Cebu Normal UniversityChelsea Wu100% (1)
- 2014 2015 2016 Student Research Compilation PDFDocumento293 pagine2014 2015 2016 Student Research Compilation PDFد.زياد الشاميNessuna valutazione finora
- Drugs For AsthmaDocumento7 pagineDrugs For Asthmaapi-3736350Nessuna valutazione finora
- Instruments UpdatepptxDocumento41 pagineInstruments UpdatepptxAshu KhanNessuna valutazione finora
- Respiratory Topic SummaryDocumento7 pagineRespiratory Topic SummaryShingie MatemaNessuna valutazione finora
- Nebulizer TherapyDocumento10 pagineNebulizer TherapyjerinthomasrajanNessuna valutazione finora
- NCP Ineffective Airway Clearance Related To The Accumulation of Secretions As Evidence by Decrease in Respiratory Rate and NGT and ET Tube Attached and Crackles at The Left Base of The LungsDocumento3 pagineNCP Ineffective Airway Clearance Related To The Accumulation of Secretions As Evidence by Decrease in Respiratory Rate and NGT and ET Tube Attached and Crackles at The Left Base of The LungsSarah Ann Jamilla FaciolanNessuna valutazione finora
- Intro To Pharmacology Study GuideDocumento93 pagineIntro To Pharmacology Study GuideMichelle Morgan LongstrethNessuna valutazione finora
- PcolDocumento17 paginePcolThea JulianaNessuna valutazione finora
- Salbutamol + IpratropiumDocumento3 pagineSalbutamol + IpratropiumShiva TorinsNessuna valutazione finora
- Case Simulation 3 in Pediatric NursingDocumento3 pagineCase Simulation 3 in Pediatric NursingCaren MarquezNessuna valutazione finora
- Gawat Darurat Paru OK RevisedDocumento121 pagineGawat Darurat Paru OK RevisedNasayu Nadia Santika AyuNessuna valutazione finora