Potrebbero piacerti anche
- The Nurse Manager Accelerator Transition from Bedside Nursing to Nurse Manager in 6 stepsDa EverandThe Nurse Manager Accelerator Transition from Bedside Nursing to Nurse Manager in 6 stepsNessuna valutazione finora
- StaffingDocumento36 pagineStaffingAshok Kumar Jangir88% (8)
- PLANNINGDocumento4 paginePLANNINGAnonymous hYMWbANessuna valutazione finora
- Establishment of Edn InstitutionDocumento88 pagineEstablishment of Edn InstitutionNise Mon KuriakoseNessuna valutazione finora
- Nightingale Institute of Nursing: AssignmentDocumento18 pagineNightingale Institute of Nursing: AssignmentDhAiRyA ArOrANessuna valutazione finora
- ICU Designing and PlanningDocumento26 pagineICU Designing and PlanningXray medicityNessuna valutazione finora
- Disaster - Mangt IVDocumento15 pagineDisaster - Mangt IVDeepti KukretiNessuna valutazione finora
- MGT 2Documento1.042 pagineMGT 2kavi kandhuNessuna valutazione finora
- Seminar On: Budget Estimate, Revised Budget and Performance Budget)Documento12 pagineSeminar On: Budget Estimate, Revised Budget and Performance Budget)Reshma AnilkumarNessuna valutazione finora
- Currents Trends in MGTDocumento23 pagineCurrents Trends in MGTsuganthi rajesh kanna100% (1)
- Calculation of Manpower of Each Category For 450 Bedded Hospital With PDFDocumento9 pagineCalculation of Manpower of Each Category For 450 Bedded Hospital With PDFamita chakraborty100% (1)
- Identify The Problems of The Speciality Units To Develop Plan of Action by Using Problem Solving AppraoachDocumento19 pagineIdentify The Problems of The Speciality Units To Develop Plan of Action by Using Problem Solving Appraoachvani reddyNessuna valutazione finora
- Maniba Bhula Nursing College: Subject: TopicDocumento11 pagineManiba Bhula Nursing College: Subject: TopicmeghanaNessuna valutazione finora
- Assignment On Staffing Pattern of Nursing Education Sub: Nursing ManagementDocumento6 pagineAssignment On Staffing Pattern of Nursing Education Sub: Nursing ManagementPrity DeviNessuna valutazione finora
- Assignment On Staffing Pattern of Hospital: Sub: Nursing ManagementDocumento6 pagineAssignment On Staffing Pattern of Hospital: Sub: Nursing ManagementPrity DeviNessuna valutazione finora
- Panna Dhai Maa Subharti Nursing College: Innovations in Nursing Amritanshu Chanchal M.SC Nursing 2nd YearDocumento31 paginePanna Dhai Maa Subharti Nursing College: Innovations in Nursing Amritanshu Chanchal M.SC Nursing 2nd YearamritanshuNessuna valutazione finora
- Inquiry ReportDocumento2 pagineInquiry ReportRuthraaadi RameshkumarNessuna valutazione finora
- Nursing ManagementDocumento12 pagineNursing ManagementFaustin RoseNessuna valutazione finora
- Nightingale Institute of Nursing, Noida: Equipment UtilizationDocumento13 pagineNightingale Institute of Nursing, Noida: Equipment UtilizationDhAiRyA ArOrANessuna valutazione finora
- Current Trend in NSG AdmDocumento17 pagineCurrent Trend in NSG AdmAnusha Verghese100% (1)
- Evaluationppt 110926211536 Phpapp01Documento35 pagineEvaluationppt 110926211536 Phpapp01Seema VashishtNessuna valutazione finora
- Evaluation Tool For Staff AppraisalDocumento7 pagineEvaluation Tool For Staff AppraisalAnusha VergheseNessuna valutazione finora
- Practical 3 PDFDocumento6 paginePractical 3 PDFPriyanjali Saini100% (1)
- Assignment On Field Appraisal ReportDocumento5 pagineAssignment On Field Appraisal ReportRenita ChrisNessuna valutazione finora
- Preparing A Budget For The Small HospitalDocumento27 paginePreparing A Budget For The Small HospitalWael100% (1)
- Progressive Patient CareDocumento2 pagineProgressive Patient Carejh_ajj100% (2)
- Seminar-Quality Assurance Correction AsirDocumento201 pagineSeminar-Quality Assurance Correction AsirASIR DHAYANINessuna valutazione finora
- Budget Proposal..Final..14.3.11Documento12 pagineBudget Proposal..Final..14.3.11Naveen EldoseNessuna valutazione finora
- En - PPR - Nursing College & School of NursingDocumento129 pagineEn - PPR - Nursing College & School of NursingDonor CrewNessuna valutazione finora
- CHN Notes VipDocumento211 pagineCHN Notes Vipyasodha maharajNessuna valutazione finora
- Nursing Audit by KaminiDocumento8 pagineNursing Audit by KaminimahiNessuna valutazione finora
- Problem Solving Approach Topic WordDocumento20 pagineProblem Solving Approach Topic Wordvani reddyNessuna valutazione finora
- 06 Physical Layout Plan of Educational InstitutionDocumento7 pagine06 Physical Layout Plan of Educational InstitutionNaveen EldoseNessuna valutazione finora
- Medical-Surgical EmergenciesDocumento78 pagineMedical-Surgical EmergenciesGopala Hari100% (8)
- Venture in NursingDocumento16 pagineVenture in NursingSabna Ajas100% (4)
- Planning and Organizing Hospital Units and Ancillary ServicesDocumento33 paginePlanning and Organizing Hospital Units and Ancillary ServicesManisha Thakur100% (1)
- PertDocumento34 paginePertVikrant ChaudharyNessuna valutazione finora
- Estimation of Nursing Staff Requirment Active Analysis and Various Research StudiesDocumento17 pagineEstimation of Nursing Staff Requirment Active Analysis and Various Research StudiesmOHAN.S100% (2)
- Presentation FPAI 2014 2Documento20 paginePresentation FPAI 2014 2Sameer Dubey0% (1)
- Planning and Organizing of HospitalDocumento36 paginePlanning and Organizing of HospitalMamta Poonia100% (1)
- Modern Techniques. in Nursing AdministrationDocumento79 pagineModern Techniques. in Nursing AdministrationSwapna Rajesh96% (24)
- Staffing Pattern Old NewDocumento5 pagineStaffing Pattern Old NewsrinivasanaNessuna valutazione finora
- Nursing Hospital Staff Job Description AimsDocumento20 pagineNursing Hospital Staff Job Description AimsSanthu Su100% (1)
- Philosophy of Hospita L 2003Documento26 paginePhilosophy of Hospita L 2003Tanu GulatiNessuna valutazione finora
- NABHDocumento14 pagineNABHdrdurgadasNessuna valutazione finora
- Nursing ManagementDocumento84 pagineNursing ManagementShiela Marie CastroNessuna valutazione finora
- Developing Staffing PattternDocumento6 pagineDeveloping Staffing PattternSharin K VargheseNessuna valutazione finora
- LDRPDocumento20 pagineLDRPAnonymous ibmeej9Nessuna valutazione finora
- Staffing of A Nursing Educational InstituteDocumento26 pagineStaffing of A Nursing Educational InstituteBaishali DebNessuna valutazione finora
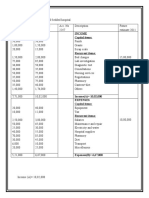
- Income Capital ItemsDocumento2 pagineIncome Capital ItemsDeepti KukretiNessuna valutazione finora
- Budget PPTDocumento15 pagineBudget PPTbushraanwarNessuna valutazione finora
- Lecture-11 HMX, Hospital BudgetDocumento43 pagineLecture-11 HMX, Hospital BudgetMuhammad Umar100% (2)
- Design Lay OutDocumento30 pagineDesign Lay Outmanish agarwal100% (6)
- 07 Job Description of Nursing Personnel in HospitalDocumento14 pagine07 Job Description of Nursing Personnel in HospitalNaveen Eldose88% (33)
- BugetDocumento13 pagineBugetDeepti Kukreti100% (1)
- QP 2012 Advanced Nursing PracticeDocumento1 paginaQP 2012 Advanced Nursing PracticeAxsa AlexNessuna valutazione finora
- Nightingale Institute of Nursing, Noida: Organizational ChartsDocumento16 pagineNightingale Institute of Nursing, Noida: Organizational ChartsDhAiRyA ArOrA100% (1)
- Staffing: Presented By:-Harpreet KaurDocumento63 pagineStaffing: Presented By:-Harpreet KaurHarpreet KaurNessuna valutazione finora
- Staffing: Click To Edit Master Subtitle Style 5/27/12 Rajesh Kumar SharmaDocumento23 pagineStaffing: Click To Edit Master Subtitle Style 5/27/12 Rajesh Kumar SharmaRajesh Kumar SharmaNessuna valutazione finora
- StaffingDocumento20 pagineStaffingmohsinayaz100% (3)
- Collective BargainingDocumento12 pagineCollective BargainingsreekalaNessuna valutazione finora
- Fowler Spiritual DevelopmentDocumento19 pagineFowler Spiritual Developmentsreekala100% (1)
- Nursing Care Plan For Master Shyne With AllDocumento17 pagineNursing Care Plan For Master Shyne With AllsreekalaNessuna valutazione finora
- Clinical Presentation On PnemoniaDocumento37 pagineClinical Presentation On PnemoniasreekalaNessuna valutazione finora
- Altered ThermoregulationDocumento29 pagineAltered Thermoregulationsreekala100% (1)
- Neonatal Seizure OriginalDocumento47 pagineNeonatal Seizure Originalsreekala100% (1)
- Social and Preventive PediatricsDocumento11 pagineSocial and Preventive PediatricssreekalaNessuna valutazione finora
- Infant of Diabetic MotherDocumento14 pagineInfant of Diabetic MothersreekalaNessuna valutazione finora
- Birth TraumaDocumento44 pagineBirth TraumasreekalaNessuna valutazione finora
- Is 456 - 2016 4th Amendment Plain and Reinforced Concrete - Code of Practice - Civil4MDocumento3 pagineIs 456 - 2016 4th Amendment Plain and Reinforced Concrete - Code of Practice - Civil4Mvasudeo_ee0% (1)
- Tool - Single Double Triple Loop LearningDocumento2 pagineTool - Single Double Triple Loop LearningDwiAryantiNessuna valutazione finora
- May 29Documento2 pagineMay 29gerrymattinglyNessuna valutazione finora
- Coronel Vs CA, GR No 103577Documento10 pagineCoronel Vs CA, GR No 103577AddAllNessuna valutazione finora
- Progress Test 1 Units 1-6: Exercise 1 Personal InformationDocumento3 pagineProgress Test 1 Units 1-6: Exercise 1 Personal InformationLuis Villaverde VerasteguiNessuna valutazione finora
- Comparative and Superlative AdjectivesDocumento11 pagineComparative and Superlative AdjectivesUri Leandro MuñozNessuna valutazione finora
- Manila Trading & Supply Co. v. Manila Trading Labor Assn (1953)Documento2 pagineManila Trading & Supply Co. v. Manila Trading Labor Assn (1953)Zan BillonesNessuna valutazione finora
- Subject: Managerial Accounting Topic: Total Quality Management Reporter: Romalyn R. PurificacionDocumento2 pagineSubject: Managerial Accounting Topic: Total Quality Management Reporter: Romalyn R. Purificacionromalyn purificacionNessuna valutazione finora
- Elements of User Interface DesignDocumento30 pagineElements of User Interface DesignRomer Garcia100% (1)
- Performance AnalyticsDocumento193 paginePerformance AnalyticsGNessuna valutazione finora
- Knowledge Versus OpinionDocumento20 pagineKnowledge Versus OpinionShumaila HameedNessuna valutazione finora
- Bay Marshalling BoxesDocumento4 pagineBay Marshalling BoxesSimbu ArasanNessuna valutazione finora
- RB September 2014 The One Thing Kekuatan Fokus Untuk Mendorong ProduktivitasDocumento2 pagineRB September 2014 The One Thing Kekuatan Fokus Untuk Mendorong ProduktivitasRifat TaopikNessuna valutazione finora
- R15 Aerodynamics Notes PDFDocumento61 pagineR15 Aerodynamics Notes PDFRahil MpNessuna valutazione finora
- Home DepotDocumento13 pagineHome DepotTyfanie PetersenNessuna valutazione finora
- The Impact of Digitalization On Business ModelsDocumento20 pagineThe Impact of Digitalization On Business ModelsFaheemullah HaddadNessuna valutazione finora
- Acute TonsillitisDocumento22 pagineAcute Tonsillitisg0ldz21100% (10)
- PM Plan Template For PresentationDocumento3 paginePM Plan Template For Presentationjamal123456Nessuna valutazione finora
- Reaction Paper PoliticsDocumento1 paginaReaction Paper PoliticsDenise Jim GalantaNessuna valutazione finora
- Amlogic USB Burning Tool V2 Guide V0.5Documento11 pagineAmlogic USB Burning Tool V2 Guide V0.5Andri R. LarekenNessuna valutazione finora
- Thomas Friedman - The World Is FlatDocumento12 pagineThomas Friedman - The World Is FlatElena ȚăpeanNessuna valutazione finora
- Case Theory BigamyDocumento6 pagineCase Theory BigamyLouem GarceniegoNessuna valutazione finora
- Jacob Marries Leah and RachelDocumento1 paginaJacob Marries Leah and RacheljellyB RafaelNessuna valutazione finora
- LESSON 1 Overview of Toeic Speaking WritingDocumento29 pagineLESSON 1 Overview of Toeic Speaking WritingPhạm Thị HuyềnNessuna valutazione finora
- TRAFFIC JUNCTION SIMULATION-projectDocumento45 pagineTRAFFIC JUNCTION SIMULATION-projectmacklyn tyan100% (2)
- Arts 9 M1 Q3 1Documento15 pagineArts 9 M1 Q3 1Gina GalvezNessuna valutazione finora
- Opening Evolution by Bill WallDocumento11 pagineOpening Evolution by Bill WallKartik ShroffNessuna valutazione finora
- SID3004 Report Writing Sep2023-CompressedDocumento39 pagineSID3004 Report Writing Sep2023-CompressedU2004743 STUDENTNessuna valutazione finora
- Bing Step by StepDocumento9 pagineBing Step by StepLaura CosteiuNessuna valutazione finora
- KISS Notes The World CommunicatesDocumento30 pagineKISS Notes The World CommunicatesJenniferBackhus100% (4)