Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- CV ArsanaDocumento2 pagineCV ArsanaAnonymous y6NmP9NHkYNessuna valutazione finora
- ManuscriptDocumento14 pagineManuscriptAnonymous y6NmP9NHkYNessuna valutazione finora
- Manuscript PDFDocumento22 pagineManuscript PDFAnonymous y6NmP9NHkYNessuna valutazione finora
- An Overview of Referral Patients With Severe Preeclampsia in Obstetric and Gynecology Department, Dr. Soetomo Hospital Surabaya in 2011 An OverviewDocumento10 pagineAn Overview of Referral Patients With Severe Preeclampsia in Obstetric and Gynecology Department, Dr. Soetomo Hospital Surabaya in 2011 An OverviewAnonymous y6NmP9NHkYNessuna valutazione finora
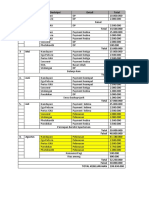
- Timeline RABDocumento1 paginaTimeline RABAnonymous y6NmP9NHkYNessuna valutazione finora
- ManuscriptDocumento17 pagineManuscriptAnonymous y6NmP9NHkYNessuna valutazione finora
- Surat Kesediaan First Author Under Review Akhir November 2018Documento6 pagineSurat Kesediaan First Author Under Review Akhir November 2018Anonymous y6NmP9NHkYNessuna valutazione finora
- Systemic Lupus Eritematus Kuliah KlerkDocumento76 pagineSystemic Lupus Eritematus Kuliah KlerkAnonymous y6NmP9NHkYNessuna valutazione finora
- Management of Spinal Injury - RON 2Documento68 pagineManagement of Spinal Injury - RON 2Anonymous y6NmP9NHkYNessuna valutazione finora
- Surat Kesediaan First Author Under Review Akhir November 2018Documento6 pagineSurat Kesediaan First Author Under Review Akhir November 2018Anonymous y6NmP9NHkYNessuna valutazione finora
- Academics Lebenslauf Vorlage ENG 0 PDFDocumento2 pagineAcademics Lebenslauf Vorlage ENG 0 PDFzana risticNessuna valutazione finora
- Contoh LoADocumento3 pagineContoh LoAAnonymous y6NmP9NHkYNessuna valutazione finora
- Curriculum Vitae: Faisal Yusuf Ashari, MDDocumento3 pagineCurriculum Vitae: Faisal Yusuf Ashari, MDAnonymous y6NmP9NHkYNessuna valutazione finora
- CV ArsanaDocumento2 pagineCV ArsanaAnonymous y6NmP9NHkYNessuna valutazione finora
- MR IRD 2014 Okt 27Documento6 pagineMR IRD 2014 Okt 27Anonymous y6NmP9NHkYNessuna valutazione finora
- Essay BTKVDocumento1 paginaEssay BTKVAnonymous y6NmP9NHkYNessuna valutazione finora
- Liflet CampakDocumento1 paginaLiflet CampakAnonymous y6NmP9NHkYNessuna valutazione finora
- Te No SynovitisDocumento47 pagineTe No SynovitisAnonymous y6NmP9NHkYNessuna valutazione finora
- Essay BTKVDocumento1 paginaEssay BTKVAnonymous y6NmP9NHkYNessuna valutazione finora
- DEPKES RI 2011 Pedoman Penanggulangan TB Di Indonesia PDFDocumento59 pagineDEPKES RI 2011 Pedoman Penanggulangan TB Di Indonesia PDFMartin Susanto, MD100% (9)
- High Tuberculosis Notification and Treatment Success Rates Through Community Participation in Central Sulawesi, Republic of IndonesiaDocumento8 pagineHigh Tuberculosis Notification and Treatment Success Rates Through Community Participation in Central Sulawesi, Republic of IndonesiaAnonymous y6NmP9NHkYNessuna valutazione finora
- Rundown Forum Presentasi CIP PEPC Th. 2015, Hotel Eastparc YogyakartaDocumento5 pagineRundown Forum Presentasi CIP PEPC Th. 2015, Hotel Eastparc YogyakartaAnonymous y6NmP9NHkYNessuna valutazione finora
- Gastrointestinal Bleeding IwkDocumento34 pagineGastrointestinal Bleeding IwkAnonymous y6NmP9NHkYNessuna valutazione finora
- Epi 1 TriangleDocumento14 pagineEpi 1 Trianglehadi_irfan8961Nessuna valutazione finora
- Water's BaruDocumento56 pagineWater's BaruAnonymous y6NmP9NHkYNessuna valutazione finora
- High Tuberculosis Notification and Treatment Success Rates Through Community Participation in Central Sulawesi, Republic of IndonesiaDocumento8 pagineHigh Tuberculosis Notification and Treatment Success Rates Through Community Participation in Central Sulawesi, Republic of IndonesiaAnonymous y6NmP9NHkYNessuna valutazione finora
- Zung ScaleDocumento2 pagineZung ScalemydepressiontestNessuna valutazione finora
- DotsDocumento6 pagineDotsAnonymous y6NmP9NHkYNessuna valutazione finora
- Final TB Screening GuidelinesDocumento146 pagineFinal TB Screening GuidelinesAnonymous y6NmP9NHkYNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Cleft Lip and PalateDocumento32 pagineCleft Lip and PalateD YasIr MussaNessuna valutazione finora
- Anat 5.2 Pelvis and Perineum - ElevazoDocumento14 pagineAnat 5.2 Pelvis and Perineum - Elevazolovelots1234Nessuna valutazione finora
- Ischemic Heart Disease Congestive Heart Failure ShockDocumento30 pagineIschemic Heart Disease Congestive Heart Failure ShockHerbert Baquerizo VargasNessuna valutazione finora
- Low Back Pain-Orthoinfo - AaosDocumento13 pagineLow Back Pain-Orthoinfo - AaosBang mantoNessuna valutazione finora
- Pages From MAF Nextcare 2Documento1 paginaPages From MAF Nextcare 2Fahad ThahaNessuna valutazione finora
- PhysioEx 2 Skeletal Muscle Physiology Worksheet Act 1 To 7Documento8 paginePhysioEx 2 Skeletal Muscle Physiology Worksheet Act 1 To 7ZHAREIGHNEILE C. MAMOLONessuna valutazione finora
- Therefore "Weakness" DOES NOT Help To Establish Whether It Is UMN or LMN lesion-FOLLOWING Pattern of Signs Help Us To EstablishDocumento66 pagineTherefore "Weakness" DOES NOT Help To Establish Whether It Is UMN or LMN lesion-FOLLOWING Pattern of Signs Help Us To EstablishBaishakhi ChakrabortyNessuna valutazione finora
- 2 - Anatomy and Histology Pearls MarchDocumento20 pagine2 - Anatomy and Histology Pearls MarchMary patrize Gonzales100% (1)
- Lesson Plan - Anatomy of Liver23Documento8 pagineLesson Plan - Anatomy of Liver23Delphy Varghese100% (1)
- Development of The MandibleDocumento9 pagineDevelopment of The MandibleHub SciNessuna valutazione finora
- Comparison Between Antegrade Nailing and Retrograde Nailing in Humeral Diaphyseal FracturesDocumento5 pagineComparison Between Antegrade Nailing and Retrograde Nailing in Humeral Diaphyseal FracturesPrabhakaran NarayanasamyNessuna valutazione finora
- Its All About The Psoas EbookDocumento25 pagineIts All About The Psoas Ebookdisegnattora67% (3)
- Difficult Airway Management: 2009 Adrian SieberhagenDocumento26 pagineDifficult Airway Management: 2009 Adrian Sieberhagendpeka dpekaNessuna valutazione finora
- Respiratory SystemDocumento13 pagineRespiratory Systemapi-270700888Nessuna valutazione finora
- Developing ToothDocumento3 pagineDeveloping ToothZHIARA MAE FACUNNessuna valutazione finora
- PID L4-L5 (Case Study)Documento67 paginePID L4-L5 (Case Study)NannieNessuna valutazione finora
- Physical Education Class 12 Chapter 6 NotesDocumento11 paginePhysical Education Class 12 Chapter 6 NotesAanchal PandeyNessuna valutazione finora
- Dry Needling Case Studies 1-5Documento13 pagineDry Needling Case Studies 1-5munesh shrivastvaNessuna valutazione finora
- Biological Basis of PersonalityDocumento58 pagineBiological Basis of PersonalityAldrian Maulion EvangelistaNessuna valutazione finora
- Spinal Manual 20 August 2004Documento235 pagineSpinal Manual 20 August 2004Forum PompieriiNessuna valutazione finora
- Manual Cervical TractionDocumento5 pagineManual Cervical TractionAritha Handrico0% (1)
- Just Go With The FlowDocumento2 pagineJust Go With The FlowIRISNessuna valutazione finora
- By Dr. Alfredo GuzmanDocumento4 pagineBy Dr. Alfredo Guzman2013SecBNessuna valutazione finora
- Piuitary DisordersDocumento40 paginePiuitary DisordersSuliman GarallehNessuna valutazione finora
- Laboratory 11Documento8 pagineLaboratory 11Jc JardinicoNessuna valutazione finora
- Breast AnatomyDocumento53 pagineBreast AnatomyShriniwas RushiNessuna valutazione finora
- Convict Conditioning Workout JournalDocumento3 pagineConvict Conditioning Workout JournalMihadNageeb100% (5)
- Physiology of INTEGUMENTARY SYSTEM FK PDFDocumento84 paginePhysiology of INTEGUMENTARY SYSTEM FK PDFdaris agharidNessuna valutazione finora
- Volkmann's Ischemic ContractureDocumento41 pagineVolkmann's Ischemic ContractureKrishna Madhukar91% (11)
- OSCE Mark Sheet 2Documento49 pagineOSCE Mark Sheet 2Niro282886% (7)