Potrebbero piacerti anche
- Pencernaan FaalDocumento82 paginePencernaan FaalhardianNessuna valutazione finora
- PulmCrit - Understanding Happy Hypoxemia PhysiologyDocumento13 paginePulmCrit - Understanding Happy Hypoxemia PhysiologyhardianNessuna valutazione finora
- Ergonomic Principles For Dental HygienistDocumento53 pagineErgonomic Principles For Dental HygienisthardianNessuna valutazione finora
- Visceral Smooth MuscleDocumento3 pagineVisceral Smooth MusclehardianNessuna valutazione finora
- Neurophysiology: Understanding How The Nervous System WorksDocumento72 pagineNeurophysiology: Understanding How The Nervous System WorkshardianNessuna valutazione finora
- Cep Crit App Web1Documento59 pagineCep Crit App Web1hardianNessuna valutazione finora
- P-LCR Parameter - Platelet Large Cell Ratio - Medical LaboratoriesDocumento3 pagineP-LCR Parameter - Platelet Large Cell Ratio - Medical LaboratorieshardianNessuna valutazione finora
- Fisiologi Sistem Saraf PusatDocumento90 pagineFisiologi Sistem Saraf PusathardianNessuna valutazione finora
- Blood and Lymphatic PhysiologyDocumento63 pagineBlood and Lymphatic PhysiologyhardianNessuna valutazione finora
- Physiology of JointsDocumento6 paginePhysiology of JointshardianNessuna valutazione finora
- Early Dementia QuestionnaireDocumento3 pagineEarly Dementia QuestionnairehardianNessuna valutazione finora
- Pathophysiology of ParesthesiaDocumento17 paginePathophysiology of Paresthesiahardian0% (1)
- Critical Appraisal of Articles About Diagnostic TestsDocumento43 pagineCritical Appraisal of Articles About Diagnostic TestshardianNessuna valutazione finora
- Assessment of Growth and Global Developmental Delay: A Study Among Young Children in A Rural Community of IndiaDocumento4 pagineAssessment of Growth and Global Developmental Delay: A Study Among Young Children in A Rural Community of IndiahardianNessuna valutazione finora
- Clinical Use of Carotid Intima-Media Thickness: Review of The LiteratureDocumento8 pagineClinical Use of Carotid Intima-Media Thickness: Review of The LiteraturehardianNessuna valutazione finora
- Archive of SID: Original ArticleDocumento5 pagineArchive of SID: Original ArticlehardianNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Lyp. Immunoassay Plus Control - Lot 40400 - ED 31 Oktober 2023Documento18 pagineLyp. Immunoassay Plus Control - Lot 40400 - ED 31 Oktober 2023Anggraeni Rismarito SihotangNessuna valutazione finora
- 3 - BIO-Describe The Feedback Mechanisms Involved in Menstrual CycleDocumento11 pagine3 - BIO-Describe The Feedback Mechanisms Involved in Menstrual CycleCarlo ThornappleNessuna valutazione finora
- Ob Supplement Handout by DR - Chris SorianoDocumento33 pagineOb Supplement Handout by DR - Chris SorianoHedley Chua75% (4)
- CTS-3 STARS Academy Multan Campus-Secure PDFDocumento14 pagineCTS-3 STARS Academy Multan Campus-Secure PDFHanzala ShahidNessuna valutazione finora
- TCM Treatment of Polycystic Ovary and PCOS: Case ReportDocumento5 pagineTCM Treatment of Polycystic Ovary and PCOS: Case ReportMarcin SowNessuna valutazione finora
- Science 10: Quarter 3 Module 2 Week 2Documento4 pagineScience 10: Quarter 3 Module 2 Week 2Adrian Orrick Capiral80% (5)
- TierneyDocumento9 pagineTierneyAna MoraisNessuna valutazione finora
- Gyne Lecture NoteDocumento572 pagineGyne Lecture NoteMRT RadiologyNessuna valutazione finora
- NEET Challenge Biology Questions - NK SharmaDocumento2 pagineNEET Challenge Biology Questions - NK SharmaMohini MalkarNessuna valutazione finora
- Notes On Subfertility AssessmentDocumento5 pagineNotes On Subfertility AssessmentHassen ZabalaNessuna valutazione finora
- Role of HormonesDocumento23 pagineRole of HormonesJhuvy C. TigbaoNessuna valutazione finora
- Bentuk Dan Fungsi Hewan: Nutrisi Yang Baik Untuk Hewan TernakDocumento10 pagineBentuk Dan Fungsi Hewan: Nutrisi Yang Baik Untuk Hewan Ternakresfani febriaNessuna valutazione finora
- 9 - Hyperandrogenemia and Insulin Resistance - The Chief Culprit of Polycystic Ovary Syndrome - 2019Documento32 pagine9 - Hyperandrogenemia and Insulin Resistance - The Chief Culprit of Polycystic Ovary Syndrome - 2019Johanna Bustos NutricionistaNessuna valutazione finora
- MenopauseDocumento21 pagineMenopauseDr K AmbareeshaNessuna valutazione finora
- Pathology Mcq's - XenoMEDDocumento11 paginePathology Mcq's - XenoMEDfreeuser3Nessuna valutazione finora
- DoReMi Ni Lalala EDITED PDFDocumento156 pagineDoReMi Ni Lalala EDITED PDFEleonor Katreeya LimsiNessuna valutazione finora
- 18 Male Hypogonadism LR1Documento24 pagine18 Male Hypogonadism LR1Retma Rosela NurkayantyNessuna valutazione finora
- Amenorrhea: An Approach To Diagnosis and ManagementDocumento8 pagineAmenorrhea: An Approach To Diagnosis and ManagementtapayanaNessuna valutazione finora
- 2nd Quarter Exam Science 10Documento11 pagine2nd Quarter Exam Science 10Brille Anthony BunielNessuna valutazione finora
- Elisa Product ListDocumento18 pagineElisa Product ListVinsmoke SanjiNessuna valutazione finora
- 14 - Toronto Notes 2011 - GynecologyDocumento52 pagine14 - Toronto Notes 2011 - GynecologyZiyad100% (4)
- Jurnal Delima Harapan 2019Documento7 pagineJurnal Delima Harapan 2019rarasindung palupiNessuna valutazione finora
- 51 Lecture The Gynecological ExamDocumento69 pagine51 Lecture The Gynecological ExamTarek TarekNessuna valutazione finora
- NCERT Solutions For Class 12 Biology Chapter 3 Human ReproductionDocumento10 pagineNCERT Solutions For Class 12 Biology Chapter 3 Human Reproductionjiya jainNessuna valutazione finora
- For Use On The IMMULITE and Immulite 1000 SystemsDocumento32 pagineFor Use On The IMMULITE and Immulite 1000 SystemsAhmed Ismail MehrimNessuna valutazione finora
- Scitec Nutrition-Catalog 2011Documento172 pagineScitec Nutrition-Catalog 2011Relu VilcuNessuna valutazione finora
- AMH and PCODocumento10 pagineAMH and PCOwaleedaliNessuna valutazione finora
- OB - TransesDocumento112 pagineOB - TransesAldwin BagtasNessuna valutazione finora
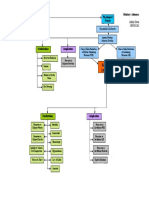
- Pituitary Adenoma Concept MapDocumento1 paginaPituitary Adenoma Concept Mapnursing concept mapsNessuna valutazione finora
- Kelompok 1 - Definisi Hormon Dan DerivatnyaDocumento17 pagineKelompok 1 - Definisi Hormon Dan DerivatnyaJihan NurainiNessuna valutazione finora