Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Resume of CasangelbabeDocumento3 pagineResume of Casangelbabeapi-28289267Nessuna valutazione finora
- Coordinators BibleDocumento60 pagineCoordinators BibleSava SánchezNessuna valutazione finora
- CPT Coding Examples For Common Spine Procedures: CervicalDocumento5 pagineCPT Coding Examples For Common Spine Procedures: CervicalKrishna KumarNessuna valutazione finora
- Money Tooth BookDocumento41 pagineMoney Tooth BookVizi Adrian0% (2)
- Current Concepts General Thoracic Surgery I To 12Documento313 pagineCurrent Concepts General Thoracic Surgery I To 12thuannguyen1219089Nessuna valutazione finora
- List of SMS 02012015Documento1 paginaList of SMS 02012015ramrai dhakerNessuna valutazione finora
- Medical Chronology Sample-MVA-Medico Legal Request LLCDocumento94 pagineMedical Chronology Sample-MVA-Medico Legal Request LLCMedico Legal Request LLCNessuna valutazione finora
- Final Physical ExaminationDocumento3 pagineFinal Physical Examinationapi-620159117Nessuna valutazione finora
- CPT © 2014 American Medical Association. All Rights ReservedDocumento2 pagineCPT © 2014 American Medical Association. All Rights ReservedtimvrghsNessuna valutazione finora
- Part 7 Pyeloroplasty: Quick and BloodlessDocumento31 paginePart 7 Pyeloroplasty: Quick and BloodlessAnonymous MmiBnqnDyNessuna valutazione finora
- 2019 - SAGE - MICS Aortic Valve Replacement With Sutureless Valves, International Prospective RegistryDocumento11 pagine2019 - SAGE - MICS Aortic Valve Replacement With Sutureless Valves, International Prospective RegistryOmán P. Jiménez A.Nessuna valutazione finora
- DR Luca Vricella Interview Transcript 1Documento19 pagineDR Luca Vricella Interview Transcript 1api-690757487Nessuna valutazione finora
- Bodybuilder Perseveres Through Physical and Emotional ObstaclesDocumento10 pagineBodybuilder Perseveres Through Physical and Emotional ObstaclesZach BermanNessuna valutazione finora
- Root Coverage PDFDocumento24 pagineRoot Coverage PDFJason Pak100% (1)
- 2 Antepartum Haemorrhage: Hannah Yeeles and Swati JhaDocumento14 pagine2 Antepartum Haemorrhage: Hannah Yeeles and Swati JhadeweNessuna valutazione finora
- Evaluation of Guaifenesin-Ketamine-Xylazine and Diazepam-Ketamine-Xylazine Triple Drip For Gelding in EquinesDocumento5 pagineEvaluation of Guaifenesin-Ketamine-Xylazine and Diazepam-Ketamine-Xylazine Triple Drip For Gelding in Equinessanjeev pitlawarNessuna valutazione finora
- American Journal of Respiratory and Critical Care MedicineDocumento12 pagineAmerican Journal of Respiratory and Critical Care MedicineChanya ChomchoeyNessuna valutazione finora
- (Transes) Human Histology - 11 Cardiovascular SystemDocumento22 pagine(Transes) Human Histology - 11 Cardiovascular SystemReina CastronuevoNessuna valutazione finora
- Mishermaliyani I11105026Documento49 pagineMishermaliyani I11105026Dewi rafikaNessuna valutazione finora
- Chapter 17 Cytology SpecimensDocumento2 pagineChapter 17 Cytology SpecimensHalidah Rahawarin100% (1)
- Adult Langerhans Cell Histiocytosis A Rare Entity in Cervical Spine Compression Case ReportDocumento4 pagineAdult Langerhans Cell Histiocytosis A Rare Entity in Cervical Spine Compression Case ReportInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Atlas of LiposuctionDocumento242 pagineAtlas of LiposuctionIvo100% (2)
- Circle of VillisDocumento17 pagineCircle of VillisAradhana SamuelNessuna valutazione finora
- Potential NCP Breast CancerDocumento3 paginePotential NCP Breast CancerMichael Oliva IIINessuna valutazione finora
- Acyanotic Congenital Heart Disease: Left-to-Right Shunt LesionsDocumento17 pagineAcyanotic Congenital Heart Disease: Left-to-Right Shunt LesionsAgustinaNessuna valutazione finora
- Panduan Troli EmergencyDocumento3 paginePanduan Troli EmergencyTukiyemNessuna valutazione finora
- Essentials of Anatomy and Physiology 5th Edition Scanlon ch01Documento28 pagineEssentials of Anatomy and Physiology 5th Edition Scanlon ch01ellieNessuna valutazione finora
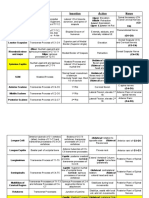
- Muscle Origins, Insertions, Actions, and InterventionsDocumento15 pagineMuscle Origins, Insertions, Actions, and InterventionsJoseph Kachelman100% (3)
- Breast Calcification - A Diagnostic ManualDocumento209 pagineBreast Calcification - A Diagnostic ManualGrace Georgina Saldana100% (3)
- DR - Jayasree.C, MBBS Resume.Documento3 pagineDR - Jayasree.C, MBBS Resume.Sathish KumarNessuna valutazione finora