Potrebbero piacerti anche
- Successful Accreditation in Echocardiography: A Self-Assessment GuideDa EverandSuccessful Accreditation in Echocardiography: A Self-Assessment GuideNessuna valutazione finora
- Hypertrophic CardiomyopathyDocumento37 pagineHypertrophic CardiomyopathyMarko Vukovic100% (1)
- Hypertrophic CardiomyopathyDocumento57 pagineHypertrophic CardiomyopathycynNessuna valutazione finora
- Hypertrophic CardiomyopathyDocumento10 pagineHypertrophic CardiomyopathySam SonNessuna valutazione finora
- Valvular Heart Disease 2Documento46 pagineValvular Heart Disease 2Topea BogdanNessuna valutazione finora
- Assessment of Right Ventricular FunctionDocumento41 pagineAssessment of Right Ventricular FunctionAditya MadhavpeddiNessuna valutazione finora
- ECG IMM 2020.docx.2Documento25 pagineECG IMM 2020.docx.2Abdul QuyyumNessuna valutazione finora
- Avnrt AvrtDocumento21 pagineAvnrt AvrtRima Rovanne Wenas100% (1)
- ECG Interpretation ECG Interpretation Basics & Quick Guide PDFDocumento157 pagineECG Interpretation ECG Interpretation Basics & Quick Guide PDFNers SenNessuna valutazione finora
- Cardiology QuestionDocumento63 pagineCardiology QuestionRazi Baik100% (1)
- ACCSAP 10 ArrhythmiaDocumento129 pagineACCSAP 10 ArrhythmiaMuhammad Javed GabaNessuna valutazione finora
- Clin Cardiology CasesDocumento34 pagineClin Cardiology CasesSunny Singh0% (1)
- 10 CardiomyopathyDocumento71 pagine10 CardiomyopathyAnonymous vUEDx8100% (5)
- Unstable Angina, STEMI, NSTEMI Diagnosis and ManagementDocumento21 pagineUnstable Angina, STEMI, NSTEMI Diagnosis and ManagementNabil Mosharraf Hossain100% (2)
- Heart Failure With Preserved Ejection FractionDocumento19 pagineHeart Failure With Preserved Ejection Fractioncosmin balanNessuna valutazione finora
- AkiDocumento20 pagineAkiEnvhy AmaliaNessuna valutazione finora
- Atrial Septal DefectDocumento12 pagineAtrial Septal DefectGassi S. PratamaNessuna valutazione finora
- Acute Renal Failure CaseDocumento4 pagineAcute Renal Failure CaseMayer RosenbergNessuna valutazione finora
- Pediatric Dilated CardiomyopathyDocumento10 paginePediatric Dilated CardiomyopathyRiduan Adoro Lumban GaolNessuna valutazione finora
- Aortic Valve DiseaseDocumento63 pagineAortic Valve DiseaseFaridOrahaNessuna valutazione finora
- Pathophysiology of Heart FailureDocumento1 paginaPathophysiology of Heart Failureiz11Nessuna valutazione finora
- Mitral Stenosis Mitral RegurgitationDocumento66 pagineMitral Stenosis Mitral RegurgitationMarshellaTriPradilagaNessuna valutazione finora
- Cerebrovascular Accident: TypesDocumento10 pagineCerebrovascular Accident: TypesJulia SalvioNessuna valutazione finora
- Clinchers 100 Important PointsDocumento21 pagineClinchers 100 Important PointsNeha GoelNessuna valutazione finora
- Pulmonary HypertensionDocumento54 paginePulmonary HypertensionpaanarNessuna valutazione finora
- ASCITESDocumento25 pagineASCITESGanesh BabuNessuna valutazione finora
- Pulmonary EmbolismDocumento4 paginePulmonary Embolismemmag1221100% (1)
- D. ST Elevations in Lead V4RDocumento4 pagineD. ST Elevations in Lead V4RDian ParamitaNessuna valutazione finora
- Clinical Exam NotesDocumento222 pagineClinical Exam NotesNarcis PopaNessuna valutazione finora
- DVT Pulmonary EmbolismDocumento40 pagineDVT Pulmonary EmbolismDr. Shatdal ChaudharyNessuna valutazione finora
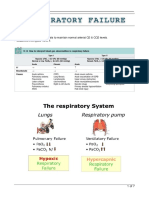
- Respiratory FailureDocumento7 pagineRespiratory FailureLulu100% (1)
- Congestive Heart FailureDocumento19 pagineCongestive Heart FailureIlavenil PanduranganNessuna valutazione finora
- Core V - Cardiovascular CoreDocumento35 pagineCore V - Cardiovascular CoreMatthew LeiNessuna valutazione finora
- ACCSAP 10 Qs & As ReviewDocumento470 pagineACCSAP 10 Qs & As ReviewAdeel Lakhiar100% (9)
- Nursing Management of Patient With Pericardial EffusionDocumento2 pagineNursing Management of Patient With Pericardial EffusionAgung Alber0% (3)
- CT Shows Diffuse Fatty Thickening of Interatrial SeptumDocumento13 pagineCT Shows Diffuse Fatty Thickening of Interatrial SeptumHaluk AlibazogluNessuna valutazione finora
- Heart Failure: Low Output HF High Output HFDocumento7 pagineHeart Failure: Low Output HF High Output HFJake BurrNessuna valutazione finora
- ACP Board Review Nephrology 20052ndDocumento35 pagineACP Board Review Nephrology 20052nddoctormido2010100% (1)
- Pathology of the Heart: Chronic Ischemic Heart Disease and Sudden Cardiac DeathDocumento11 paginePathology of the Heart: Chronic Ischemic Heart Disease and Sudden Cardiac DeathIsabel CastilloNessuna valutazione finora
- 101 Cases PDFDocumento412 pagine101 Cases PDFWilliamPresley100% (1)
- INOTROPESDocumento8 pagineINOTROPESessevyNessuna valutazione finora
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocumento15 pagineCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoNessuna valutazione finora
- Blood and Drugs Medicine NotesDocumento39 pagineBlood and Drugs Medicine Notesrahuul prasadNessuna valutazione finora
- 2d Speckle Tracking Echocardiography PDFDocumento11 pagine2d Speckle Tracking Echocardiography PDFYEAG92100% (1)
- Accsap 10 VHDDocumento94 pagineAccsap 10 VHDMuhammad Javed Gaba100% (2)
- Valvular Heart DiseaseDocumento10 pagineValvular Heart DiseaseEzyan SyaminNessuna valutazione finora
- ACC Cardiovascular Board Review MCQ 2017Documento64 pagineACC Cardiovascular Board Review MCQ 2017Adeel Lakhiar100% (1)
- Pediatric Pharmacology: Dr. Putrya Hawa, M.Biomed Faculty of Medicine, UIIDocumento27 paginePediatric Pharmacology: Dr. Putrya Hawa, M.Biomed Faculty of Medicine, UIIAfied Fitrah100% (1)
- Peripheral Vascular Disease Arteries NHSDocumento10 paginePeripheral Vascular Disease Arteries NHSAdahl HetheringtonNessuna valutazione finora
- Hypertension LecturesDocumento65 pagineHypertension LecturesAdebisiNessuna valutazione finora
- Diagnosis and Assessment of Acute StrokesDocumento22 pagineDiagnosis and Assessment of Acute Strokesyulian100% (2)
- ECG Master Class-3Documento97 pagineECG Master Class-3Shohag ID CenterNessuna valutazione finora
- Congestive Heart FailureDocumento86 pagineCongestive Heart FailureNabeel ShahzadNessuna valutazione finora
- Valvular Heart DiseaseDocumento2 pagineValvular Heart DiseaseAnonymous TVk12eX4Nessuna valutazione finora
- MCQ Cardio 3Documento50 pagineMCQ Cardio 3Dian ParamitaNessuna valutazione finora
- Valvular Heart DiseaseDocumento54 pagineValvular Heart DiseaseKiki RizkyNessuna valutazione finora
- Nuclear CardiologyDocumento4 pagineNuclear CardiologysivaNessuna valutazione finora
- Bedside Cardiology (2012) (PDF)Documento251 pagineBedside Cardiology (2012) (PDF)Loredana Dobrea100% (4)
- Ischemic Heart DiseaseDocumento28 pagineIschemic Heart DiseaseLiusHarimanNessuna valutazione finora
- 3t SMP Ut Cable AssyDocumento8 pagine3t SMP Ut Cable Assymsmith6477Nessuna valutazione finora
- 555 Timer and Its Applications (M.C. Sharma)Documento48 pagine555 Timer and Its Applications (M.C. Sharma)victorhugoserranoNessuna valutazione finora
- Murray Model 465306x8a Garden Tractor (2004) Parts ListDocumento17 pagineMurray Model 465306x8a Garden Tractor (2004) Parts Listmsmith6477Nessuna valutazione finora
- Code Check - BuildingDocumento34 pagineCode Check - BuildingYongHyu ParkNessuna valutazione finora
- Pemeriksaan LabDocumento1 paginaPemeriksaan LabYeri HoloNessuna valutazione finora
- Yin I KnowltonDocumento14 pagineYin I KnowltonFrancesco Gubby GubinelliNessuna valutazione finora
- Murray Model 465306x8a Garden Tractor (2004) Parts ListDocumento17 pagineMurray Model 465306x8a Garden Tractor (2004) Parts Listmsmith6477Nessuna valutazione finora
- HP Jan04 ThyroidDocumento2 pagineHP Jan04 Thyroidmsmith6477Nessuna valutazione finora
- Murray Model 465306x8a Garden Tractor (2004) Parts ListDocumento17 pagineMurray Model 465306x8a Garden Tractor (2004) Parts Listmsmith6477Nessuna valutazione finora
- Pemeriksaan LabDocumento1 paginaPemeriksaan LabYeri HoloNessuna valutazione finora
- The Differential Diagnosis of FatigueDocumento4 pagineThe Differential Diagnosis of Fatiguemsmith6477Nessuna valutazione finora
- Heart DiseaseDocumento15 pagineHeart Diseasemsmith6477Nessuna valutazione finora
- 209-208 Pancreas DiseasesDocumento14 pagine209-208 Pancreas Diseasesmsmith6477Nessuna valutazione finora
- 4513 7806 1 PBDocumento7 pagine4513 7806 1 PBmsmith6477Nessuna valutazione finora
- Data Sheet Acquired From Harris Semiconductor SCHS030D Revised December 2003Documento23 pagineData Sheet Acquired From Harris Semiconductor SCHS030D Revised December 2003msmith6477Nessuna valutazione finora
- Training Heating Gas Valve SystemsDocumento62 pagineTraining Heating Gas Valve Systemsphild2na2Nessuna valutazione finora
- Acca Manual J and D Mechanical RequirementsDocumento1 paginaAcca Manual J and D Mechanical Requirementsmsmith6477Nessuna valutazione finora
- Atmel 11209 32 Bit Cortex M4 Microcontroller SAM G51 DatasheetDocumento866 pagineAtmel 11209 32 Bit Cortex M4 Microcontroller SAM G51 Datasheetmsmith6477Nessuna valutazione finora
- Acca Manual J and D Mechanical RequirementsDocumento1 paginaAcca Manual J and D Mechanical Requirementsmsmith6477Nessuna valutazione finora
- Chap 04 BDocumento26 pagineChap 04 Bmsmith6477Nessuna valutazione finora
- CAM Diagnosis and Management of DeliriumDocumento1 paginaCAM Diagnosis and Management of Deliriummsmith6477Nessuna valutazione finora
- Baird Chapter 1Documento26 pagineBaird Chapter 1msmith6477Nessuna valutazione finora
- Router Modle Number 315.17560Documento12 pagineRouter Modle Number 315.17560msmith6477Nessuna valutazione finora
- The Confusion Assessment Method (CAM) Diagnostic Algorithm: Other Than "Alert"Documento1 paginaThe Confusion Assessment Method (CAM) Diagnostic Algorithm: Other Than "Alert"msmith6477Nessuna valutazione finora
- CAM Diagnosis and Management of DeliriumDocumento1 paginaCAM Diagnosis and Management of Deliriummsmith6477Nessuna valutazione finora
- r4f Pastest MnemonicsDocumento23 paginer4f Pastest MnemonicsplayuhzNessuna valutazione finora
- EBARA FS513CT-R0E pump manualDocumento6 pagineEBARA FS513CT-R0E pump manualApriliyanto Rahadi PradanaNessuna valutazione finora
- Mic ProjectDocumento12 pagineMic Projectsarthakjoshi012Nessuna valutazione finora
- Divide and Conquer (Closest Pair, Convex Hull, Strassen Matrix Multiply) DemoDocumento27 pagineDivide and Conquer (Closest Pair, Convex Hull, Strassen Matrix Multiply) DemoAnand KumarNessuna valutazione finora
- LearnEnglish Video Zone How These Women Changed Science ForeverDocumento3 pagineLearnEnglish Video Zone How These Women Changed Science ForeverDaniella MensatoNessuna valutazione finora
- Manual de Uso Ecografo GE Logiq e PDFDocumento192 pagineManual de Uso Ecografo GE Logiq e PDFDaniel CortesNessuna valutazione finora
- Instrukcja Pellets Fuzzy Logic - ENGDocumento53 pagineInstrukcja Pellets Fuzzy Logic - ENGxilef84Nessuna valutazione finora
- Tenofovir Disoproxil Fumarate: Riefing - Nfrared BsorptionDocumento4 pagineTenofovir Disoproxil Fumarate: Riefing - Nfrared BsorptionMostofa RubalNessuna valutazione finora
- Lea 2 PDFDocumento21 pagineLea 2 PDFKY Renz100% (1)
- Poisoning: Selenium in LivestockDocumento4 paginePoisoning: Selenium in Livestockdianarbk otuNessuna valutazione finora
- Unchained MelodeeDocumento93 pagineUnchained MelodeeRafael Cornholio RodriguezNessuna valutazione finora
- Pitfalls of HIV Infection - Dr. Rizqi Amalia, Sp.ADocumento46 paginePitfalls of HIV Infection - Dr. Rizqi Amalia, Sp.AandreknhNessuna valutazione finora
- Grade 9 Unit 1 - Part 1: Square RootsDocumento20 pagineGrade 9 Unit 1 - Part 1: Square RootsWilson ZhangNessuna valutazione finora
- Error Correction - Test 1Documento4 pagineError Correction - Test 1phucnguyen0429Nessuna valutazione finora
- 43-101 Technical Report Quimsacocha, February 2009Documento187 pagine43-101 Technical Report Quimsacocha, February 2009Marco Vinicio SotoNessuna valutazione finora
- Steam Turbine Unloading and Shut-Down of Operation Turbine/Generator Shut-Down Diagram (General)Documento1 paginaSteam Turbine Unloading and Shut-Down of Operation Turbine/Generator Shut-Down Diagram (General)parthibanemails5779Nessuna valutazione finora
- 2023-05-11 St. Mary's County TimesDocumento40 pagine2023-05-11 St. Mary's County TimesSouthern Maryland OnlineNessuna valutazione finora
- Fossil Fuel and The Environment PPT Project FinalDocumento14 pagineFossil Fuel and The Environment PPT Project Finalapi-298052133Nessuna valutazione finora
- SPECIFIC GRAVITY - DENSITY OF HYDRAULIC CEMENT (IS - 4031-Part 11-1988)Documento6 pagineSPECIFIC GRAVITY - DENSITY OF HYDRAULIC CEMENT (IS - 4031-Part 11-1988)Pritha DasNessuna valutazione finora
- Etabloc Technical DataDocumento108 pagineEtabloc Technical Dataedward ksbNessuna valutazione finora
- The Anglican Digest - Winter 2022Documento64 pagineThe Anglican Digest - Winter 2022The Anglican Digest100% (1)
- Real Talk GrammarDocumento237 pagineReal Talk GrammarOmar yoshiNessuna valutazione finora
- Vedic Astrology OverviewDocumento1 paginaVedic Astrology Overviewhuman999100% (8)
- داينمك الملزمة كاملةDocumento79 pagineداينمك الملزمة كاملةarno assassin33% (3)
- Swami Brahmananda - The Spiritual Son of Sri RamakrishnaDocumento7 pagineSwami Brahmananda - The Spiritual Son of Sri RamakrishnaEstudante da Vedanta100% (2)
- Sdre14-5 Ral 1-2-Rev17Documento3 pagineSdre14-5 Ral 1-2-Rev17lwin_oo2435Nessuna valutazione finora
- 3-Ph Induction MotorDocumento246 pagine3-Ph Induction MotorAn00pgadzillaNessuna valutazione finora
- STPM Chemistry Topic 16 Haloalkanes Short Notes PDFDocumento2 pagineSTPM Chemistry Topic 16 Haloalkanes Short Notes PDFbendanNessuna valutazione finora
- Koh Pich Construction Company Cambodia-China Polytechnic University Daily Activities ReportDocumento7 pagineKoh Pich Construction Company Cambodia-China Polytechnic University Daily Activities ReportNhoek RenNessuna valutazione finora
- National Leprosy Control Program For CHNDocumento18 pagineNational Leprosy Control Program For CHNNaomi Cyden YapNessuna valutazione finora
- Dr. Carlos S. Lanting College: College of Maritime EducationDocumento14 pagineDr. Carlos S. Lanting College: College of Maritime EducationJeynard Moler J. TanNessuna valutazione finora