Potrebbero piacerti anche
- Intravenous TherapyDocumento30 pagineIntravenous TherapyKoass14 2012Nessuna valutazione finora
- IV Therapy SlidesDocumento8 pagineIV Therapy SlidesRegean MercadoNessuna valutazione finora
- Blood Transfusion: Registered Nurses To Transfuse Blood. As A New Graduate Be Sure To Access YourDocumento9 pagineBlood Transfusion: Registered Nurses To Transfuse Blood. As A New Graduate Be Sure To Access YourPriya YadavNessuna valutazione finora
- Blood Transfusion: By: Dr. Hira HanifDocumento51 pagineBlood Transfusion: By: Dr. Hira HanifTariq sattarNessuna valutazione finora
- IV TherapyDocumento39 pagineIV TherapyRichard SiahaanNessuna valutazione finora
- Revalida 1Documento3 pagineRevalida 1herrabiel solisNessuna valutazione finora
- HemorrhageProtocol TableChart v1.4Documento1 paginaHemorrhageProtocol TableChart v1.4manleyj5305Nessuna valutazione finora
- Upper GI BleedDocumento50 pagineUpper GI BleedNiladri BanerjeeNessuna valutazione finora
- Meds-Study GuideDocumento3 pagineMeds-Study Guidejackli21Nessuna valutazione finora
- Icnc Audit FaqDocumento12 pagineIcnc Audit FaqtarunikinaraNessuna valutazione finora
- Perioperative Fluid TherapyDocumento36 paginePerioperative Fluid TherapyUmhy GumianaNessuna valutazione finora
- Tricuspid Pulmonic Mitral Aortic: Purpose: Blood Products Including Whole Blood or Packed Red Blood CellsDocumento42 pagineTricuspid Pulmonic Mitral Aortic: Purpose: Blood Products Including Whole Blood or Packed Red Blood CellsYieNessuna valutazione finora
- 1-3 - IV TherapyDocumento17 pagine1-3 - IV TherapyjaikovskyNessuna valutazione finora
- Hemodynamic MonitoringDocumento4 pagineHemodynamic Monitoringgurneet kourNessuna valutazione finora
- Electrolyte ImbalanceDocumento47 pagineElectrolyte ImbalanceKaye Nicole LugoNessuna valutazione finora
- Blood TranfusionDocumento37 pagineBlood TranfusionRaras P P100% (1)
- ATI IV TherapyDocumento8 pagineATI IV Therapylisa100% (1)
- Intravenous Infusion and Blood TransfusionDocumento21 pagineIntravenous Infusion and Blood Transfusioncamaralamin209_54266Nessuna valutazione finora
- 4.massive HemorrhageDocumento44 pagine4.massive HemorrhageyeabsraNessuna valutazione finora
- IVT NotesDocumento5 pagineIVT NotesChared LumbaNessuna valutazione finora
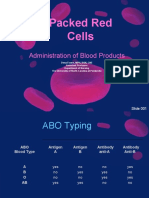
- Packed Red Cells: Administration of Blood ProductsDocumento36 paginePacked Red Cells: Administration of Blood ProductsRj SantosNessuna valutazione finora
- Reaksi TransfusiDocumento5 pagineReaksi TransfusiInatrinNessuna valutazione finora
- El Tiempo Es Vida. Haga Lo Correcto, en El Momento Adecuado ...Documento23 pagineEl Tiempo Es Vida. Haga Lo Correcto, en El Momento Adecuado ...Emilio Fernandez CenturiónNessuna valutazione finora
- Wardclass Powerpoint Blood TransfusionDocumento27 pagineWardclass Powerpoint Blood TransfusionKatherine 'Chingboo' Leonico Laud60% (5)
- Upper Gastrointestinal BleedingDocumento41 pagineUpper Gastrointestinal BleedingAnusha VergheseNessuna valutazione finora
- Sepsis Management: Runal Shah 1 Year Resident MEM, Kdah, MumbaiDocumento18 pagineSepsis Management: Runal Shah 1 Year Resident MEM, Kdah, Mumbaibotet_2306Nessuna valutazione finora
- Central Venous PressureDocumento22 pagineCentral Venous Pressurejhong100% (1)
- Anesthesia For Kidney TransplantDocumento6 pagineAnesthesia For Kidney TransplantachyutsharmaNessuna valutazione finora
- Exchange TransfusionDocumento9 pagineExchange TransfusiondewpraNessuna valutazione finora
- Blood TransfusionDocumento29 pagineBlood TransfusionNonu Kims100% (1)
- Atul Sharma Uppergi Fcccm23Documento47 pagineAtul Sharma Uppergi Fcccm23Atul SharmaNessuna valutazione finora
- Transfusi DarahDocumento33 pagineTransfusi DarahnengninisNessuna valutazione finora
- Intravenous Fluid Therapy: Paramedic ClassDocumento48 pagineIntravenous Fluid Therapy: Paramedic ClassBon Joey BernestoNessuna valutazione finora
- 145 278 1 SMDocumento28 pagine145 278 1 SMAtika RosmiaNessuna valutazione finora
- Neonatal Exchange TransfusionDocumento33 pagineNeonatal Exchange TransfusionedrinsneNessuna valutazione finora
- Blood TransfusionDocumento28 pagineBlood TransfusionDrmirfat AlkashifNessuna valutazione finora
- Central Venous Pressure MonitoringDocumento3 pagineCentral Venous Pressure MonitoringJulienne Sanchez-SalazarNessuna valutazione finora
- Pulmonary Edema, Hypotension, or Shock AlgorithmDocumento34 paginePulmonary Edema, Hypotension, or Shock AlgorithmMuhammad SafaatNessuna valutazione finora
- Lecture 4: Hypovolemic ShockDocumento20 pagineLecture 4: Hypovolemic Shockj.doe.hex_87Nessuna valutazione finora
- Darah ManusiaaDocumento1 paginaDarah ManusiaaTcacolate Telsa ElizsabethNessuna valutazione finora
- Transfusion Reactions CHDocumento22 pagineTransfusion Reactions CHHenni Wahyu TriyuniatiNessuna valutazione finora
- Shock: Mazen Kherallah, MD, FCCPDocumento38 pagineShock: Mazen Kherallah, MD, FCCPPatrick KosgeiNessuna valutazione finora
- Transfusi DarahDocumento33 pagineTransfusi DarahDwi Cahayani UtamiNessuna valutazione finora
- Blood TransfusionDocumento5 pagineBlood TransfusionAngie Doctolero100% (1)
- Introduction To Intravenous InfusionDocumento8 pagineIntroduction To Intravenous Infusionblndnazi3279Nessuna valutazione finora
- DVT ProphylaxisDocumento30 pagineDVT ProphylaxisedhsnzktNessuna valutazione finora
- Transfusion Process For NursesDocumento31 pagineTransfusion Process For NursesShoheb ShaikhNessuna valutazione finora
- CVP ReportDocumento37 pagineCVP ReportJulienne Sanchez-SalazarNessuna valutazione finora
- Abdominal TraumaDocumento39 pagineAbdominal TraumaMuvenn KannanNessuna valutazione finora
- OctaplexDocumento3 pagineOctaplexraul sinatoNessuna valutazione finora
- Abnormal PeurpuriumDocumento25 pagineAbnormal Peurpuriumjanuna63Nessuna valutazione finora
- Assessment of the Politraumatized PatientDa EverandAssessment of the Politraumatized PatientNessuna valutazione finora
- Transfusion Medicine and Hemostasis: Clinical and Laboratory AspectsDa EverandTransfusion Medicine and Hemostasis: Clinical and Laboratory AspectsValutazione: 4 su 5 stelle4/5 (9)
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingDa EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNessuna valutazione finora
- Alert Medical Series: Emergency Medicine Alert IIIDa EverandAlert Medical Series: Emergency Medicine Alert IIINessuna valutazione finora
- Thesis 101 Presence of HazardsDocumento2 pagineThesis 101 Presence of HazardsNecesario BanaagNessuna valutazione finora
- Educational Attainment: X. Socio-Cultural IndicesDocumento13 pagineEducational Attainment: X. Socio-Cultural IndicesNecesario BanaagNessuna valutazione finora
- Significance of The StudyDocumento1 paginaSignificance of The StudyNecesario BanaagNessuna valutazione finora
- Final Gordon'SFunctionalHealthDocumento4 pagineFinal Gordon'SFunctionalHealthNecesario BanaagNessuna valutazione finora
- FHNDocumento45 pagineFHNNecesario BanaagNessuna valutazione finora
- Fatima 121 ThesisDocumento144 pagineFatima 121 ThesisNecesario BanaagNessuna valutazione finora
- IntroductionDocumento2 pagineIntroductionNecesario BanaagNessuna valutazione finora
- Chapter 14 HandoutsDocumento10 pagineChapter 14 HandoutsNecesario BanaagNessuna valutazione finora
- 2Ce-D Jersey: Name Subtot Al 11-Jul 12-Jul 13-Jul 14-Jul 15-Jul 16-Jul 19-Jul T2Documento2 pagine2Ce-D Jersey: Name Subtot Al 11-Jul 12-Jul 13-Jul 14-Jul 15-Jul 16-Jul 19-Jul T2Necesario BanaagNessuna valutazione finora
- Patent Ductus Arteriosus (PDA) Is A Congenital Heart Defect Wherein The Ductus Arteriosus FailsDocumento2 paginePatent Ductus Arteriosus (PDA) Is A Congenital Heart Defect Wherein The Ductus Arteriosus FailsNecesario BanaagNessuna valutazione finora
- Problem PrioritizationDocumento4 pagineProblem PrioritizationNecesario BanaagNessuna valutazione finora
- Puro Sito LogiaDocumento77 paginePuro Sito LogiaNecesario BanaagNessuna valutazione finora
- Kashmir Life 12.3Documento24 pagineKashmir Life 12.3im hepNessuna valutazione finora
- Rhesus Blood Group SystemDocumento4 pagineRhesus Blood Group SystemNahyanNessuna valutazione finora
- Chapter 7 RH Blood Group SystemDocumento28 pagineChapter 7 RH Blood Group Systemschemology100% (1)
- Laboratory Tests and Diagnostic ProceduresDocumento21 pagineLaboratory Tests and Diagnostic Procedurestostc33% (3)
- Hypersensitivity: M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM UniversityDocumento87 pagineHypersensitivity: M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM UniversityJulienne Sanchez-SalazarNessuna valutazione finora
- Clinical Laboratory Immunology 1st Edition Maahon Tice Test BankDocumento8 pagineClinical Laboratory Immunology 1st Edition Maahon Tice Test BankBrian Craig100% (37)
- AIIMS May 2003 Questions and AnswersDocumento32 pagineAIIMS May 2003 Questions and AnswersSayeed KhanNessuna valutazione finora
- Blood ProductDocumento89 pagineBlood ProductSam0% (1)
- KLB Biology F3 NoteDocumento49 pagineKLB Biology F3 NoteSocdal AbdiNessuna valutazione finora
- Biology M14 Genetics - The Study of Inherited TraitsDocumento33 pagineBiology M14 Genetics - The Study of Inherited TraitsDiana Dealino-SabandalNessuna valutazione finora
- Lesson 7 y 8Documento23 pagineLesson 7 y 8Eugenia GonzalezNessuna valutazione finora
- RH Incompatibility Case StudyDocumento14 pagineRH Incompatibility Case StudyMary Beth AbelidoNessuna valutazione finora
- Minutes of Meeting On Blood TransfusionDocumento3 pagineMinutes of Meeting On Blood TransfusionJeezreelNessuna valutazione finora
- Blood ComponentsDocumento101 pagineBlood ComponentsNyxa AbdullaNessuna valutazione finora
- FREE NLE REVIEW Np2Documento38 pagineFREE NLE REVIEW Np2Charm LigawadNessuna valutazione finora
- 5BBK Lec5 - Other Blood Groups MQA 2019-09-26 08-14-44Documento37 pagine5BBK Lec5 - Other Blood Groups MQA 2019-09-26 08-14-44gothai sivapragasamNessuna valutazione finora
- Forensic Chemistry & ToxicologyDocumento139 pagineForensic Chemistry & ToxicologyMelcon S. Lapina93% (28)
- Memon Medical Institute Hospital: Laboratory Rate ListDocumento26 pagineMemon Medical Institute Hospital: Laboratory Rate List1123456789000% (1)
- Math All QuarterDocumento324 pagineMath All Quarteralvin madahanNessuna valutazione finora
- Smart Blood Bank: Quadrilateral Health / FitnessDocumento20 pagineSmart Blood Bank: Quadrilateral Health / FitnessYuktiNessuna valutazione finora
- Medical Lab TechnicianDocumento47 pagineMedical Lab Techniciandrzaur50% (4)
- Sci-Tech QuizDocumento72 pagineSci-Tech QuizKing GamerNessuna valutazione finora
- Form 3 CH 3Documento91 pagineForm 3 CH 3amalina rohaizan100% (2)
- Hmis in Blood BanksDocumento35 pagineHmis in Blood BanksDrPriyanka Prashant PawsheNessuna valutazione finora
- Forensic Laboratory: Department of Forensic Medicine Faculty of Medicine Udayana UniversityDocumento78 pagineForensic Laboratory: Department of Forensic Medicine Faculty of Medicine Udayana UniversityHananya ManroeNessuna valutazione finora
- Abo Blood Group Part 1Documento23 pagineAbo Blood Group Part 1Alanah JaneNessuna valutazione finora
- Argumentative EssayDocumento24 pagineArgumentative EssayLiu166Nessuna valutazione finora
- Blood BankDocumento92 pagineBlood BankDoc PreetiNessuna valutazione finora
- Human Blood GroupsDocumento29 pagineHuman Blood GroupsKunalNessuna valutazione finora
- 3 - Training Module For Blood Bank Nurses - Split - 1Documento100 pagine3 - Training Module For Blood Bank Nurses - Split - 1YousraajNessuna valutazione finora