Potrebbero piacerti anche
- Draft For Preterm LaborDocumento31 pagineDraft For Preterm LaborKimberly Jose100% (1)
- Entamoeba HistolyticaDocumento10 pagineEntamoeba HistolyticamarkNessuna valutazione finora
- Drug StudyDocumento4 pagineDrug StudyRudelsa Agcolicol LangamanNessuna valutazione finora
- Acute Bronchitis FALALALALADocumento42 pagineAcute Bronchitis FALALALALANikko MelencionNessuna valutazione finora
- MCN Drill 1Documento23 pagineMCN Drill 1Cai Velasco DecenaNessuna valutazione finora
- CretinismDocumento15 pagineCretinismJoshua fuentesNessuna valutazione finora
- Drug Study:: Prednisone Heartburn Sweating AcneDocumento7 pagineDrug Study:: Prednisone Heartburn Sweating AcneSandie Daniel GabalunosNessuna valutazione finora
- Drugs Affecting Reproductive System: Presented By: BSN 2A Group 1Documento34 pagineDrugs Affecting Reproductive System: Presented By: BSN 2A Group 1David BernalNessuna valutazione finora
- PHC Community DiagnosisDocumento27 paginePHC Community DiagnosisCassandra_Maca_6324Nessuna valutazione finora
- Urinary Catheter InsertionDocumento4 pagineUrinary Catheter InsertionAngel SamonteNessuna valutazione finora
- DiphtheriaDocumento18 pagineDiphtheriaShishir ShresthaNessuna valutazione finora
- MyocarditisDocumento1 paginaMyocarditisintrovoyz041Nessuna valutazione finora
- Hands Only CPR Instructions Sheet FinalDocumento1 paginaHands Only CPR Instructions Sheet Finalapi-472726244Nessuna valutazione finora
- Outbreak InvestigationDocumento47 pagineOutbreak Investigationsarguss14100% (1)
- CS - UTI, Acute Bronchitis, Acute GastritisDocumento39 pagineCS - UTI, Acute Bronchitis, Acute GastritisGrace BernadetteNessuna valutazione finora
- Wee Bag, Nebulization, and Oxygen Therapy ChecklistDocumento2 pagineWee Bag, Nebulization, and Oxygen Therapy Checklistapril marquesesNessuna valutazione finora
- Test Taking NLEDocumento4 pagineTest Taking NLEJayvee AmpoNessuna valutazione finora
- Placenta Abruptio: Maneja, Jan Michael B. BSN 223Documento6 paginePlacenta Abruptio: Maneja, Jan Michael B. BSN 223JiraGonzales100% (1)
- Cardiac TamponadeDocumento6 pagineCardiac TamponadeJara Maris Moreno BudionganNessuna valutazione finora
- Anthropometric MeasurementDocumento2 pagineAnthropometric MeasurementJames ClarkNessuna valutazione finora
- BreastfeedingDocumento111 pagineBreastfeedingabdur rahman zulkifliNessuna valutazione finora
- Describing The System: Components and TermsDocumento3 pagineDescribing The System: Components and TermsimnasNessuna valutazione finora
- Medical Ward - Discharge PlanDocumento5 pagineMedical Ward - Discharge Plandon7dane100% (1)
- Case Study - SisDocumento14 pagineCase Study - Sisclara_wenceslaoNessuna valutazione finora
- Pre Term LaborDocumento3 paginePre Term LaborHazel Marie Echavez100% (1)
- Administering Vaginal InstillationsDocumento6 pagineAdministering Vaginal InstillationsRudy DuterteNessuna valutazione finora
- Nursing Management During Labor and BirthDocumento23 pagineNursing Management During Labor and BirthShiella May Edquibal0% (1)
- Care of The Mother and The FetusDocumento99 pagineCare of The Mother and The FetusBea Bianca CruzNessuna valutazione finora
- Ethical Issues of Students Online Learning Environment in University of Nueva CaceresDocumento15 pagineEthical Issues of Students Online Learning Environment in University of Nueva CaceresChristian Zuela AgpoonNessuna valutazione finora
- Drug Study - Caloy PartDocumento3 pagineDrug Study - Caloy PartCarlos LleverNessuna valutazione finora
- Nursing Care Plan For The Woman at Risk For DEFICIENT FLUID VOLUME1Documento2 pagineNursing Care Plan For The Woman at Risk For DEFICIENT FLUID VOLUME1Ellie GartungNessuna valutazione finora
- Principles of Aseptic TechniqueDocumento3 paginePrinciples of Aseptic TechniqueDane CaumeranNessuna valutazione finora
- 20 Ethico-Legal Considerations and IssuesDocumento18 pagine20 Ethico-Legal Considerations and IssuesBea Bianca CruzNessuna valutazione finora
- Drug Study Clindamycin, Ipatropium BromideDocumento8 pagineDrug Study Clindamycin, Ipatropium Bromidepaupaulala100% (2)
- Immediate Hemolytic Transfusion ReactionDocumento2 pagineImmediate Hemolytic Transfusion ReactionleoNessuna valutazione finora
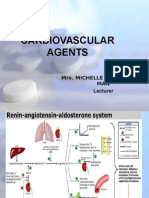
- Cardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerDocumento131 pagineCardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerNiala AlmarioNessuna valutazione finora
- NCM Renal DisordersDocumento72 pagineNCM Renal DisordersYep Yep100% (1)
- Nephrotic SyndromeDocumento37 pagineNephrotic SyndromeJon Adonis GozunNessuna valutazione finora
- BRH Drug StudyDocumento6 pagineBRH Drug StudyStephanie Dellera AgdanNessuna valutazione finora
- Drug Calculations: Making It EasyDocumento26 pagineDrug Calculations: Making It EasyShaells JoshiNessuna valutazione finora
- Cesarean Section HennawyDocumento89 pagineCesarean Section Hennawykhadzx100% (2)
- AnaestheticsDocumento33 pagineAnaestheticsAsif Ali LashariNessuna valutazione finora
- Competency-Based Training in Basic Emergency Obstetric and Newborn Care (BEmONC) Improves Provider's Performance in TanzaniaDocumento16 pagineCompetency-Based Training in Basic Emergency Obstetric and Newborn Care (BEmONC) Improves Provider's Performance in TanzaniaJhpiego100% (2)
- Intrapartum: Delivery Room Technique PurposeDocumento7 pagineIntrapartum: Delivery Room Technique Purposesharmena harunNessuna valutazione finora
- Intrapartal PeriodDocumento2 pagineIntrapartal PeriodLeah ElizabethNessuna valutazione finora
- Hirschsprung DiseaseDocumento25 pagineHirschsprung DiseaseMuhammad Zaniar RamadhaniNessuna valutazione finora
- DrowningDocumento17 pagineDrowningMAHFUZ ISLAM0% (1)
- CVP MonitoringDocumento36 pagineCVP MonitoringFlorence SanchezNessuna valutazione finora
- H MoleDocumento23 pagineH MoleJoel Santos100% (1)
- Community Diagnosis (2) RLEDocumento25 pagineCommunity Diagnosis (2) RLEAnon NimosNessuna valutazione finora
- PneumoniaDocumento17 paginePneumoniaapi-2758635670% (1)
- ImpetigoDocumento11 pagineImpetigoShailendra RijalNessuna valutazione finora
- There Are Safe Methods To Prevent Pregnancy After Unprotected SexDocumento8 pagineThere Are Safe Methods To Prevent Pregnancy After Unprotected SexRajnish Ranjan PrasadNessuna valutazione finora
- O&G Off-Tag Assesment Logbook: Traces-Pdf-248732173Documento9 pagineO&G Off-Tag Assesment Logbook: Traces-Pdf-248732173niwasNessuna valutazione finora
- CME PRETERM LABOR, PROM, PPROM FDocumento39 pagineCME PRETERM LABOR, PROM, PPROM FRatna Setia WatiNessuna valutazione finora
- Diphereline S.R 3.75mg EngDocumento3 pagineDiphereline S.R 3.75mg EngBotond BarthaNessuna valutazione finora
- Preeklamsia 1Documento32 paginePreeklamsia 1lilik hunainahNessuna valutazione finora
- Clinical OSCE With AnswersDocumento95 pagineClinical OSCE With AnswersPrasad HewawasamNessuna valutazione finora
- Essential Obstetric Care: Quality Ante Natal CareDocumento6 pagineEssential Obstetric Care: Quality Ante Natal CareMaguNessuna valutazione finora
- Gynecology All 2Documento71 pagineGynecology All 2Hikufe JesayaNessuna valutazione finora
- The Most Common (Autosaved) in OtolaryngologyDocumento15 pagineThe Most Common (Autosaved) in OtolaryngologyDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Paranasal Sinus (Repaired) EntDocumento48 pagineParanasal Sinus (Repaired) EntDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Ramsay Hunt Syndrome EntDocumento3 pagineRamsay Hunt Syndrome EntDr-Firas Nayf Al-Thawabia100% (1)
- Neonatal Facial Nerve Palsy PDFDocumento5 pagineNeonatal Facial Nerve Palsy PDFDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Facial Nerve Surgical ApproachesDocumento4 pagineFacial Nerve Surgical ApproachesDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Radiotherapy in OtolaryngologyDocumento11 pagineRadiotherapy in OtolaryngologyDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Lazer in OtolaryngologyDocumento2 pagineLazer in OtolaryngologyDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- AJCC Cancer Staging Form Supplement PDFDocumento520 pagineAJCC Cancer Staging Form Supplement PDFopi akbarNessuna valutazione finora
- CSF RhinorrheaDocumento10 pagineCSF RhinorrheaDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Neonate FN PalsyDocumento5 pagineNeonate FN PalsyDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Tracheostomy EmergenciesDocumento32 pagineTracheostomy EmergenciesDr-Firas Nayf Al-Thawabia100% (1)
- CT Imaging of The Temporal Bone: An Anatomical Review With Illustrative Cases of CholesteatomasDocumento116 pagineCT Imaging of The Temporal Bone: An Anatomical Review With Illustrative Cases of CholesteatomasDr-Firas Nayf Al-Thawabia100% (1)
- Juvenile Nasopharyngial AngiofibromaDocumento8 pagineJuvenile Nasopharyngial AngiofibromaDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Facial Nerve Surgical ApproachesDocumento4 pagineFacial Nerve Surgical ApproachesDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- MCQ S For StudentsDocumento58 pagineMCQ S For StudentsJohn M. Hemsworth100% (2)
- Zaghal 2014 - Anatomy of Facial Nerve and Tympanic AnnulusDocumento5 pagineZaghal 2014 - Anatomy of Facial Nerve and Tympanic AnnulusDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Facial Nerve Trauma: Maisa AlsmadiDocumento28 pagineFacial Nerve Trauma: Maisa AlsmadiDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Bell's PalsyDocumento9 pagineBell's PalsyDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- SR8 Regulations - OtolaryngologyDocumento4 pagineSR8 Regulations - OtolaryngologyDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Zaghal 2014 - Anatomy of Facial Nerve and Tympanic AnnulusDocumento5 pagineZaghal 2014 - Anatomy of Facial Nerve and Tympanic AnnulusDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Trauma: Accidental Temporal Bone Fractures Classification SchemesDocumento12 pagineTrauma: Accidental Temporal Bone Fractures Classification SchemesDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- HRCT Temporal Bone AnatomyDocumento66 pagineHRCT Temporal Bone AnatomyDr-Firas Nayf Al-Thawabia100% (1)
- Traumatic Facial Nerve PalsyDocumento12 pagineTraumatic Facial Nerve PalsyDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Temporalbone 151227031114Documento350 pagineTemporalbone 151227031114Dr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Allergic Rhinitiseditedppt2614Documento43 pagineAllergic Rhinitiseditedppt2614Dr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- 105.fullcong NasalDocumento12 pagine105.fullcong NasalDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Allergic Rhinitis: S PandeyDocumento37 pagineAllergic Rhinitis: S PandeyDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Allergic RhinitisDocumento38 pagineAllergic RhinitisDr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Allergicrhinitis 140911185124 Phpapp01Documento24 pagineAllergicrhinitis 140911185124 Phpapp01Dr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Pedi Nasal Mass Slides 060607Documento54 paginePedi Nasal Mass Slides 060607Dr-Firas Nayf Al-ThawabiaNessuna valutazione finora
- Activity On Lesson 2 Common Injuries in DanceDocumento10 pagineActivity On Lesson 2 Common Injuries in DancePammy AlivenNessuna valutazione finora
- Alan Immerman - Health Unlimitred PDFDocumento95 pagineAlan Immerman - Health Unlimitred PDFHMNessuna valutazione finora
- JAT - CHT 13Documento68 pagineJAT - CHT 13j_smith24Nessuna valutazione finora
- Exam Labor ProcessDocumento4 pagineExam Labor ProcessAileen A. Monares0% (1)
- Module 7 Anxiety Disorders PDFDocumento12 pagineModule 7 Anxiety Disorders PDFprashansha kumudNessuna valutazione finora
- Written Case StudyDocumento16 pagineWritten Case Studyapi-234402582Nessuna valutazione finora
- Test Bank For Equipment Theory For Respiratory Care 5th Edition by WhiteDocumento11 pagineTest Bank For Equipment Theory For Respiratory Care 5th Edition by Whiteharoldbrownorcnxeijgd100% (29)
- Focus Diagnosis Action Response Subjective: "I Hate Water and I Don't Drink It Much " DXDocumento2 pagineFocus Diagnosis Action Response Subjective: "I Hate Water and I Don't Drink It Much " DXGrape Juice100% (1)
- Avian Product Dosage Instructions Jun2017Documento4 pagineAvian Product Dosage Instructions Jun2017vetthamilNessuna valutazione finora
- Nursing Care Plan Using This Format: Prioritization of Nursing DiagnosisDocumento2 pagineNursing Care Plan Using This Format: Prioritization of Nursing DiagnosisERIKA ANNE CADAWANNessuna valutazione finora
- Hayya Moph QLMDocumento4 pagineHayya Moph QLMrrthamadNessuna valutazione finora
- GuideDocumento52 pagineGuidemihaelklajner100% (1)
- Full Report-Disinfectant and SanitizerDocumento19 pagineFull Report-Disinfectant and Sanitizermohd addinNessuna valutazione finora
- Strategic Intervention Materials PresentationDocumento55 pagineStrategic Intervention Materials PresentationMary Athena Ibardaloza Adesna100% (15)
- QSE6034: Teknologi Dan Inovasi Dalam Sains SukanDocumento3 pagineQSE6034: Teknologi Dan Inovasi Dalam Sains SukanMohamad Ramlan RamliNessuna valutazione finora
- 5 Weight LossDocumento41 pagine5 Weight LossTasniiem KhmbataNessuna valutazione finora
- Assisting Arterial Blood Gas: Lesson PlanDocumento2 pagineAssisting Arterial Blood Gas: Lesson PlanSwapnil MahapureNessuna valutazione finora
- Cardiac Risk AssessmentDocumento4 pagineCardiac Risk Assessmentmonir61Nessuna valutazione finora
- Pre Eclampsia Blood TestDocumento2 paginePre Eclampsia Blood TestAbhishek RampalNessuna valutazione finora
- Induksi Persalinan - NewDocumento20 pagineInduksi Persalinan - NewnilajmasptnaNessuna valutazione finora
- Contraceptive Injection PDFDocumento2 pagineContraceptive Injection PDFCostin VrabieNessuna valutazione finora
- სტაბილური სტენოკარდია - გაიდლაინიDocumento59 pagineსტაბილური სტენოკარდია - გაიდლაინიMikheil KakhidzeNessuna valutazione finora
- K - 9 Urinary Tract Infection (Ilmu Penyakit Dalam)Documento24 pagineK - 9 Urinary Tract Infection (Ilmu Penyakit Dalam)Ruthra Devi NarayanasamyNessuna valutazione finora
- II-Vocab of Hospital DeptDocumento1 paginaII-Vocab of Hospital DeptAdhwaNessuna valutazione finora
- Red LesionsDocumento87 pagineRed LesionsPadmaja VootlaNessuna valutazione finora
- Morning ReportDocumento31 pagineMorning Reports1882Nessuna valutazione finora
- Methods of Nutrient DeliveryDocumento3 pagineMethods of Nutrient DeliveryFarmisa MannanNessuna valutazione finora
- Epilepsy and Pregnancy Gynae Course 2013Documento57 pagineEpilepsy and Pregnancy Gynae Course 2013Anas KhanNessuna valutazione finora
- Chap-2 Notes For Clinical Nutrition and DieteticsDocumento5 pagineChap-2 Notes For Clinical Nutrition and Dieteticsstar “Hjaljimmer” platinumNessuna valutazione finora
- Herpes Zoster: Shingles Acute Posterior GanglionitisDocumento23 pagineHerpes Zoster: Shingles Acute Posterior GanglionitisHannah Clarisse Monge IgniNessuna valutazione finora
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisDa EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisValutazione: 3 su 5 stelle3/5 (2)
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayDa EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayValutazione: 5 su 5 stelle5/5 (2)
- Labor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodDa EverandLabor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodValutazione: 4.5 su 5 stelle4.5/5 (28)
- ADHD Women: A Holistic Approach To ADHD ManagementDa EverandADHD Women: A Holistic Approach To ADHD ManagementValutazione: 5 su 5 stelle5/5 (4)
- Breaking Free from Body Shame: Dare to Reclaim What God Has Named GoodDa EverandBreaking Free from Body Shame: Dare to Reclaim What God Has Named GoodValutazione: 5 su 5 stelle5/5 (33)
- What to Expect When You’re Expecting (5th Edition)Da EverandWhat to Expect When You’re Expecting (5th Edition)Valutazione: 5 su 5 stelle5/5 (1)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeDa EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeValutazione: 3.5 su 5 stelle3.5/5 (13)
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeDa EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeNessuna valutazione finora
- Awakening Fertility: The Essential Art of Preparing for PregnancyDa EverandAwakening Fertility: The Essential Art of Preparing for PregnancyValutazione: 4.5 su 5 stelle4.5/5 (36)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.Da EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Valutazione: 4.5 su 5 stelle4.5/5 (124)
- The Fifth Vital Sign: Master Your Cycles & Optimize Your FertilityDa EverandThe Fifth Vital Sign: Master Your Cycles & Optimize Your FertilityValutazione: 4.5 su 5 stelle4.5/5 (12)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouDa EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNessuna valutazione finora
- Spirit Baby: Communicate with Your Unborn Baby. Ease Your BirthDa EverandSpirit Baby: Communicate with Your Unborn Baby. Ease Your BirthValutazione: 5 su 5 stelle5/5 (1)
- I'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionDa EverandI'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionValutazione: 4.5 su 5 stelle4.5/5 (124)
- Women, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainDa EverandWomen, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainValutazione: 4 su 5 stelle4/5 (14)
- Younger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondDa EverandYounger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondValutazione: 4 su 5 stelle4/5 (110)
- Awakening Fertility: The Essential Art of Preparing for PregnancyDa EverandAwakening Fertility: The Essential Art of Preparing for PregnancyValutazione: 5 su 5 stelle5/5 (4)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondDa EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondValutazione: 4.5 su 5 stelle4.5/5 (38)
- What No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodDa EverandWhat No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodValutazione: 4.5 su 5 stelle4.5/5 (30)
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenDa EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenValutazione: 4 su 5 stelle4/5 (154)
- The Strength and Conditioning Bible: How to Train Like an AthleteDa EverandThe Strength and Conditioning Bible: How to Train Like an AthleteNessuna valutazione finora
- The Menopause Manifesto: Own Your Health With Facts and FeminismDa EverandThe Menopause Manifesto: Own Your Health With Facts and FeminismValutazione: 4 su 5 stelle4/5 (18)
- Medical Bondage: Race, Gender, and the Origins of American GynecologyDa EverandMedical Bondage: Race, Gender, and the Origins of American GynecologyValutazione: 4.5 su 5 stelle4.5/5 (75)
- Perfectly Imperfect: Your complete guide to loving yourself and loving your bodyDa EverandPerfectly Imperfect: Your complete guide to loving yourself and loving your bodyValutazione: 5 su 5 stelle5/5 (1)
- The Spark Factor: The Secret to Supercharging Energy, Becoming Resilient, and Feeling Better Than EverDa EverandThe Spark Factor: The Secret to Supercharging Energy, Becoming Resilient, and Feeling Better Than EverValutazione: 4 su 5 stelle4/5 (2)
- 9 Months Is Not Enough: The Ultimate Pre-Pregnancy Checklist to Create a Baby-Ready Body and Build Generational HealthDa Everand9 Months Is Not Enough: The Ultimate Pre-Pregnancy Checklist to Create a Baby-Ready Body and Build Generational HealthNessuna valutazione finora
- Women, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainDa EverandWomen, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainValutazione: 3.5 su 5 stelle3.5/5 (4)
- Rediscover Your Sparkle: Nourish Your SoulDa EverandRediscover Your Sparkle: Nourish Your SoulValutazione: 4.5 su 5 stelle4.5/5 (4)
- The Mama Natural Week-by-Week Guide to Pregnancy and ChildbirthDa EverandThe Mama Natural Week-by-Week Guide to Pregnancy and ChildbirthValutazione: 4.5 su 5 stelle4.5/5 (21)