Potrebbero piacerti anche
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsDa EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNessuna valutazione finora
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesDa EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesValutazione: 4 su 5 stelle4/5 (2)
- Hand Mudras For DiabetesDocumento5 pagineHand Mudras For DiabetesRITESH SINGHNessuna valutazione finora
- Insulin and Antidiabetic Drugs: Prof - DR Asya RehmanDocumento23 pagineInsulin and Antidiabetic Drugs: Prof - DR Asya RehmanGareth BaleNessuna valutazione finora
- Diabetes MellitusDocumento181 pagineDiabetes MellitusrogerNessuna valutazione finora
- Pathophysiology of DiabetesDocumento88 paginePathophysiology of DiabetesCahya SetiyaNessuna valutazione finora
- Unit 5 Part 2 InsulinDocumento68 pagineUnit 5 Part 2 InsulinKhairunnisa Loqman100% (1)
- DIABETESDocumento29 pagineDIABETESVinnes Ann InfanteNessuna valutazione finora
- NURSING PRACTICE I - Foundation of PROFESSIONAL Nursing Practice SITUATIONALDocumento102 pagineNURSING PRACTICE I - Foundation of PROFESSIONAL Nursing Practice SITUATIONALAlyssa BusalpaNessuna valutazione finora
- Case Study of Diabetes MellitusDocumento19 pagineCase Study of Diabetes Mellituschai delgadoNessuna valutazione finora
- NCLEX RN Practice Questions 17Documento29 pagineNCLEX RN Practice Questions 17clarheena89% (9)
- Perinatal Care Manual 3rd Edition 2013Documento251 paginePerinatal Care Manual 3rd Edition 2013Anonymous 9dVZCnTXS100% (3)
- Diabetic Kidney DiseaseDocumento22 pagineDiabetic Kidney Diseasenadyamulya100% (1)
- Diabetes MellitusDocumento16 pagineDiabetes MellitusApril Joy V. QuinoNessuna valutazione finora
- Pre Gestational ConditionsDocumento17 paginePre Gestational Conditionslarissedeleon100% (2)
- Smoothies for Diabetics: Reverse Diabetes and Lower Blood Sugar with 36 Quick & Easy Delicious Diabetic Smoothie RecipesDa EverandSmoothies for Diabetics: Reverse Diabetes and Lower Blood Sugar with 36 Quick & Easy Delicious Diabetic Smoothie RecipesValutazione: 5 su 5 stelle5/5 (2)
- Big Fat LieDocumento11 pagineBig Fat LieSquinkleNessuna valutazione finora
- Insulin Secretion and FunctionDocumento8 pagineInsulin Secretion and FunctionWendy EscalanteNessuna valutazione finora
- Diabetes Mellitus Final SibiDocumento62 pagineDiabetes Mellitus Final SibiSibi JohnNessuna valutazione finora
- Liver Triad Mastery - Dr. JackDocumento48 pagineLiver Triad Mastery - Dr. Jackjuststuddy100% (2)
- Diabetes Mellitus: Presented By-Deepanshi Masih 1 Year M.Sc. Nursing EconDocumento34 pagineDiabetes Mellitus: Presented By-Deepanshi Masih 1 Year M.Sc. Nursing EconAru VermaNessuna valutazione finora
- DIABETES MELLITUS FinalDocumento83 pagineDIABETES MELLITUS FinalYuvi Yuvaraj100% (1)
- CCDocumento9 pagineCCFritzie BlancheNessuna valutazione finora
- Nursing Care PlansDocumento14 pagineNursing Care PlansTels Dela PeñaNessuna valutazione finora
- Diabetes MellitusDocumento181 pagineDiabetes Mellitusnursereview95% (19)
- Newer Insulin in Diabetic Pregnancy - PPT'Documento56 pagineNewer Insulin in Diabetic Pregnancy - PPT'Hemamalini100% (1)
- Diabetes Diet Plan: Diabetic Diet Guidelines for Curing Diabetes and Lose Weight Naturally. (Diabetes Diet Cookbook and Recipes to Prevent Diabetes, Boost Metabolism , Diabetes Treatment, Diabetes TipDa EverandDiabetes Diet Plan: Diabetic Diet Guidelines for Curing Diabetes and Lose Weight Naturally. (Diabetes Diet Cookbook and Recipes to Prevent Diabetes, Boost Metabolism , Diabetes Treatment, Diabetes TipNessuna valutazione finora
- Diabetic Recipes for One and TwoDa EverandDiabetic Recipes for One and TwoValutazione: 3 su 5 stelle3/5 (1)
- Update On Childhood Diabetes MellitusDocumento51 pagineUpdate On Childhood Diabetes MellitusJulie Carnetion DNessuna valutazione finora
- C C C CDocumento51 pagineC C C CpixiemedicNessuna valutazione finora
- Diabetes Mellitus Prepared By: LORI R. LARA, R.NDocumento14 pagineDiabetes Mellitus Prepared By: LORI R. LARA, R.NNovie Carla0% (1)
- Childhood Diabetes 2016Documento64 pagineChildhood Diabetes 2016Awatef AbushhiwaNessuna valutazione finora
- Diabetes MelitusDocumento27 pagineDiabetes Melitusana chasanahNessuna valutazione finora
- Type 1 Diabetes Mellitus: EtiologyDocumento9 pagineType 1 Diabetes Mellitus: EtiologyChristian diorNessuna valutazione finora
- Paeda DMDocumento38 paginePaeda DMAmanuel LemiNessuna valutazione finora
- Diabetes OutlineDocumento7 pagineDiabetes OutlineJenny VargheseNessuna valutazione finora
- Common Endocrine Disorders: Iril I. Panes, RN, MANDocumento63 pagineCommon Endocrine Disorders: Iril I. Panes, RN, MANJona Phie Domingo MonteroNessuna valutazione finora
- 23 Diabetes MellitusDocumento19 pagine23 Diabetes Mellitusزياد سعيدNessuna valutazione finora
- DM Presentation NewDocumento44 pagineDM Presentation NewKipz JonsNessuna valutazione finora
- Diabete Mellitus HandoutsDocumento7 pagineDiabete Mellitus HandoutsSittie Nashieva A. UsmanNessuna valutazione finora
- DM Report1Documento16 pagineDM Report1Wendy EscalanteNessuna valutazione finora
- Food, Nutrition and Dietetics.: TopicDocumento8 pagineFood, Nutrition and Dietetics.: TopicT-7502 SAMITA BANERJEENessuna valutazione finora
- DiabetesmellitusDocumento24 pagineDiabetesmellitusSania SaeedNessuna valutazione finora
- Lewis: Medical-Surgical Nursing, 10 Edition: Diabetes Mellitus Key PointsDocumento6 pagineLewis: Medical-Surgical Nursing, 10 Edition: Diabetes Mellitus Key PointsDeo FactuarNessuna valutazione finora
- T31 - Types of Diabetes and Diagnosis - PTPDocumento6 pagineT31 - Types of Diabetes and Diagnosis - PTPangela adelantarNessuna valutazione finora
- DM ReportDocumento16 pagineDM ReportWendy EscalanteNessuna valutazione finora
- E SystemDocumento81 pagineE SystemErsido SamuelNessuna valutazione finora
- Diabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMDocumento20 pagineDiabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMPriyanka Karnik100% (1)
- DiabetesDocumento10 pagineDiabetesLyNessuna valutazione finora
- DMDocumento20 pagineDMKC PalattaoNessuna valutazione finora
- 12 Nursing Managment of Childern With Endocarine Disorders 2nd SemesterDocumento27 pagine12 Nursing Managment of Childern With Endocarine Disorders 2nd SemesterFaisal M.AlruwailiNessuna valutazione finora
- Diabetes MellitusDocumento6 pagineDiabetes MellituscrisrimartNessuna valutazione finora
- Diabetes NotesDocumento10 pagineDiabetes Notestripj33Nessuna valutazione finora
- MS3 Review NotesDocumento11 pagineMS3 Review NotesPaul Anthony LoricaNessuna valutazione finora
- Diabetes MellitusDocumento22 pagineDiabetes MellitusAnburaj JamesNessuna valutazione finora
- Pancreatic HormonesDocumento41 paginePancreatic HormonesBodea Doru100% (1)
- DR - Rihab Pediatrics 02.pediatric DM Part TwoDocumento7 pagineDR - Rihab Pediatrics 02.pediatric DM Part TwoMujtaba JawadNessuna valutazione finora
- Diabetes Millitus PDFDocumento41 pagineDiabetes Millitus PDFAbdullah BhattiNessuna valutazione finora
- Diabetes - Oral KnowledgeDocumento19 pagineDiabetes - Oral KnowledgeKSeegurNessuna valutazione finora
- Lesson 15: Drugs For Diabetes: Introduction (ILO-1 - 2)Documento38 pagineLesson 15: Drugs For Diabetes: Introduction (ILO-1 - 2)Ralp ManglicmotNessuna valutazione finora
- DM Case Study - Nursing CribDocumento6 pagineDM Case Study - Nursing CribFrancis VillanuevaNessuna valutazione finora
- Case Study of DMDocumento6 pagineCase Study of DMbuzz Q0% (1)
- Diabetes Mellitus Type 11Documento44 pagineDiabetes Mellitus Type 11MARICRIS NEBIARNessuna valutazione finora
- Wepik Understanding Diabetes Mellitus A Comprehensive Analysis of Causes Management and Prevention 20231126074011dxZFDocumento15 pagineWepik Understanding Diabetes Mellitus A Comprehensive Analysis of Causes Management and Prevention 20231126074011dxZFtripathyabinash39Nessuna valutazione finora
- Practical Biochemistry: Number of Experiment: (1) Name of Exp.:-Blood Glucose TestDocumento6 paginePractical Biochemistry: Number of Experiment: (1) Name of Exp.:-Blood Glucose TestHiba EmadNessuna valutazione finora
- Diabetes Mellitus Bahasa InggrisDocumento16 pagineDiabetes Mellitus Bahasa InggrisyustikapupenNessuna valutazione finora
- Ultimate Diet Plan for Diabetic Patients: Revolutionizing Diabetic NutritionDa EverandUltimate Diet Plan for Diabetic Patients: Revolutionizing Diabetic NutritionNessuna valutazione finora
- Breaking the Chains of Diabetes. A Comprehensive Guide to Understanding and Managing Diabetes NaturallyDa EverandBreaking the Chains of Diabetes. A Comprehensive Guide to Understanding and Managing Diabetes NaturallyNessuna valutazione finora
- Effect of Coffe & Stress With The Incidedence of GastritisDocumento5 pagineEffect of Coffe & Stress With The Incidedence of GastritisJufran, R (2018)Nessuna valutazione finora
- Psoriasis Treated Acetonii) E AND Occlusive Dressings: With Topical FluocinoloneDocumento2 paginePsoriasis Treated Acetonii) E AND Occlusive Dressings: With Topical FluocinoloneAndrew Surya Putra SccNessuna valutazione finora
- 608751Documento8 pagine608751adesamboraNessuna valutazione finora
- THE Canadian Medical Association: Associate, Department of Dermatology, Vancouver General Hospital, Vancouver, B.CDocumento5 pagineTHE Canadian Medical Association: Associate, Department of Dermatology, Vancouver General Hospital, Vancouver, B.CAndrew Surya Putra SccNessuna valutazione finora
- THE Canadian Medical Association: Associate, Department of Dermatology, Vancouver General Hospital, Vancouver, B.CDocumento5 pagineTHE Canadian Medical Association: Associate, Department of Dermatology, Vancouver General Hospital, Vancouver, B.CAndrew Surya Putra SccNessuna valutazione finora
- Paper No.2 ModifiedDocumento6 paginePaper No.2 ModifiedAndrew Surya Putra SccNessuna valutazione finora
- 608751Documento8 pagine608751adesamboraNessuna valutazione finora
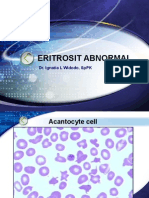
- Eritrosit AbnormalDocumento20 pagineEritrosit AbnormalAndrew Surya Putra SccNessuna valutazione finora
- Diabetes Mellitus965Documento98 pagineDiabetes Mellitus965Andrew Surya Putra SccNessuna valutazione finora
- Dkamanagment 150323150043 Conversion Gate01Documento28 pagineDkamanagment 150323150043 Conversion Gate01Andrew Surya Putra SccNessuna valutazione finora
- Slide UrineDocumento15 pagineSlide UrineAndrew Surya Putra SccNessuna valutazione finora
- Dka Pathphysiologymanagement2014 Copy 140202235658 Phpapp02Documento31 pagineDka Pathphysiologymanagement2014 Copy 140202235658 Phpapp02Andrew Surya Putra SccNessuna valutazione finora
- Eritrosit Hipokrom Mikrositer, Pencil CellDocumento6 pagineEritrosit Hipokrom Mikrositer, Pencil CellAndrew Surya Putra SccNessuna valutazione finora
- Dka Pathphysiologymanagement2014 Copy 140202235658 Phpapp02Documento31 pagineDka Pathphysiologymanagement2014 Copy 140202235658 Phpapp02Andrew Surya Putra SccNessuna valutazione finora
- CVM 00288tDocumento6 pagineCVM 00288tAndrew Surya Putra SccNessuna valutazione finora
- DKADocumento12 pagineDKAAisha SyedNessuna valutazione finora
- Diabetic Ketoacidosis: Abdelaziz Elamin Professor of Pediatric Endocrinology University of Khartoum, SudanDocumento33 pagineDiabetic Ketoacidosis: Abdelaziz Elamin Professor of Pediatric Endocrinology University of Khartoum, SudanboyzbanjarboyzNessuna valutazione finora
- CVM 00288tDocumento6 pagineCVM 00288tAndrew Surya Putra SccNessuna valutazione finora
- Pathophysiology of Atrial FibrillationDocumento12 paginePathophysiology of Atrial FibrillationAndrew Surya Putra SccNessuna valutazione finora
- DkaDocumento23 pagineDkaAnissa tri acintyaNessuna valutazione finora
- Bab 8 Daftar PustakaDocumento10 pagineBab 8 Daftar PustakaAndrew Surya Putra SccNessuna valutazione finora
- CVM 00288tDocumento6 pagineCVM 00288tAndrew Surya Putra SccNessuna valutazione finora
- Afib Info SheetDocumento2 pagineAfib Info Sheetapi-265745737Nessuna valutazione finora
- ReferenceDocumento8 pagineReferenceAndrew Surya Putra SccNessuna valutazione finora
- 0065Documento4 pagine0065Andrew Surya Putra SccNessuna valutazione finora
- Atrial Fibrillation: The Management of Atrial Fibrillation: Issued: June 2014 Last Modified: August 2014Documento50 pagineAtrial Fibrillation: The Management of Atrial Fibrillation: Issued: June 2014 Last Modified: August 2014Andrew Surya Putra SccNessuna valutazione finora
- ORBIT Guidelines Poster AHA v2-EmilyOBrien-SUNDAY - 9amDocumento1 paginaORBIT Guidelines Poster AHA v2-EmilyOBrien-SUNDAY - 9amAndrew Surya Putra SccNessuna valutazione finora
- Bab 8 Daftar PustakaDocumento10 pagineBab 8 Daftar PustakaAndrew Surya Putra SccNessuna valutazione finora
- Topical Cyclosporine in The Treatment of Allergic ConjunctivitisDocumento7 pagineTopical Cyclosporine in The Treatment of Allergic ConjunctivitisRandy AninditoNessuna valutazione finora
- Foundation of PROFESSIONAL Nursing Practice: Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDocumento19 pagineFoundation of PROFESSIONAL Nursing Practice: Practice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralNessuna valutazione finora
- ICD DiabetesDocumento4 pagineICD DiabetesfadhilahNessuna valutazione finora
- Endocrine EmergenciesDocumento25 pagineEndocrine EmergenciesayaNessuna valutazione finora
- HonkDocumento1 paginaHonkIndah Puspita Sari PaneNessuna valutazione finora
- Issue 29 - Volume 2Documento32 pagineIssue 29 - Volume 2Indian WeekenderNessuna valutazione finora
- Diabetes Resommendations Laboratory AnalysisDocumento120 pagineDiabetes Resommendations Laboratory AnalysisAleja Coneja BonifazNessuna valutazione finora
- 4 - Health Consequences of Obesity 2012Documento5 pagine4 - Health Consequences of Obesity 2012Mateus CarvalhoNessuna valutazione finora
- (Citrus Aurantium) Orange Peels and (Citrus) Lemon Extract As A Cure To Open Wound DiseaseDocumento8 pagine(Citrus Aurantium) Orange Peels and (Citrus) Lemon Extract As A Cure To Open Wound DiseaseNikko Pananganan DajaoNessuna valutazione finora
- Lagundi Tea For Stronger Lungs and LiverDocumento2 pagineLagundi Tea For Stronger Lungs and LiverJohn Mark LedesmaNessuna valutazione finora
- 14 - Blood Glucose HomeostasisDocumento34 pagine14 - Blood Glucose HomeostasischeckmateNessuna valutazione finora
- Shahid Athar, MD, FACP, Face Author, "Islamic Perspective in Medicine" (ATP)Documento25 pagineShahid Athar, MD, FACP, Face Author, "Islamic Perspective in Medicine" (ATP)She JocelynNessuna valutazione finora
- Concept PaperDocumento12 pagineConcept Paperjlventigan100% (1)
- ResearchDocumento50 pagineResearchKirtiNessuna valutazione finora
- Yoga Mudras To Reduce The Effects of DiabetesDocumento6 pagineYoga Mudras To Reduce The Effects of DiabetesAmmienus MarcellinNessuna valutazione finora
- 49 91 1 SMDocumento3 pagine49 91 1 SMFirjin LowingNessuna valutazione finora
- Blood Glucose Practical Handout For 2nd Year MBBSDocumento10 pagineBlood Glucose Practical Handout For 2nd Year MBBSIMDCBiochemNessuna valutazione finora
- Type 1 Case Study21Documento10 pagineType 1 Case Study21api-271779479Nessuna valutazione finora
- 2.0 Reasons Why Fast Food Should Be Banned 2.1 Fast Food Will Give An Impact On Human HealthDocumento4 pagine2.0 Reasons Why Fast Food Should Be Banned 2.1 Fast Food Will Give An Impact On Human HealthMichelle LiNessuna valutazione finora
- Diabetes Type I Powerpoint 2Documento10 pagineDiabetes Type I Powerpoint 2api-317440960Nessuna valutazione finora