Potrebbero piacerti anche
- Hodgkin Lymphoma: Dr. G Sirisha M.D Assistant Professor Department of Pathology, GMC, SrikakulamDocumento41 pagineHodgkin Lymphoma: Dr. G Sirisha M.D Assistant Professor Department of Pathology, GMC, SrikakulamDevisriNessuna valutazione finora
- Haematology-Pdf - 1Documento91 pagineHaematology-Pdf - 1shreyNessuna valutazione finora
- Tuberculous Lymphadenitis & Lymphoma: Prof - Dr.S.P.Gayathre Chief of General Surgery Madras Medical CollegeDocumento51 pagineTuberculous Lymphadenitis & Lymphoma: Prof - Dr.S.P.Gayathre Chief of General Surgery Madras Medical CollegeAashmi ChandrikaaNessuna valutazione finora
- Lymphoid DisordersDocumento44 pagineLymphoid DisorderssaketNessuna valutazione finora
- Lymphoreticular FinalDocumento42 pagineLymphoreticular FinalNafis Fuad SheikhNessuna valutazione finora
- Haematological Malignancies: Dr. Maruf Bin Habib Associate Professor of Medicine UamcDocumento54 pagineHaematological Malignancies: Dr. Maruf Bin Habib Associate Professor of Medicine UamcSaifSeddikiNessuna valutazione finora
- LeukemiasDocumento31 pagineLeukemiasIsaac MwangiNessuna valutazione finora
- WBC DisordersDocumento45 pagineWBC DisordersyalahopaNessuna valutazione finora
- CML, CLLDocumento118 pagineCML, CLLMunesh SherawatNessuna valutazione finora
- Chapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusDocumento10 pagineChapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusAgnieszka WisniewskaNessuna valutazione finora
- Pediatric Ent MalignanciesDocumento69 paginePediatric Ent MalignanciesKita kitaNessuna valutazione finora
- Peripheral LymphadenopathyDocumento11 paginePeripheral LymphadenopathyserubimNessuna valutazione finora
- Lymphoma: David Lee MD, FRCPCDocumento36 pagineLymphoma: David Lee MD, FRCPCQasim AliNessuna valutazione finora
- Week 15-Mature-Lymphoid-Neoplasms-SCDocumento65 pagineWeek 15-Mature-Lymphoid-Neoplasms-SCKyle CollladoNessuna valutazione finora
- Myeloproliferative NeoplasmsDocumento59 pagineMyeloproliferative NeoplasmssaketNessuna valutazione finora
- LymphomasDocumento34 pagineLymphomasanimesh vaidyaNessuna valutazione finora
- Limfoma PPT MonceDocumento65 pagineLimfoma PPT MonceSylvia PertiwiNessuna valutazione finora
- Chronic Lymphoproliferative DisordersDocumento108 pagineChronic Lymphoproliferative DisordersSiti NurrazanNessuna valutazione finora
- Hodgkins Lymphoma: DR Swathi R KrishnaDocumento83 pagineHodgkins Lymphoma: DR Swathi R KrishnaSwathi R KrishnaNessuna valutazione finora
- Leukamia and Transfusion MedicineDocumento26 pagineLeukamia and Transfusion MedicineSamuel kuriaNessuna valutazione finora
- LeukemiaDocumento51 pagineLeukemiaKailash KhatriNessuna valutazione finora
- Malig HaemDocumento47 pagineMalig HaemNisini ImanyaNessuna valutazione finora
- Lymphoma/LCH in Children: Simon BomkenDocumento45 pagineLymphoma/LCH in Children: Simon BomkenmiauNessuna valutazione finora
- Leukocyte DisordersDocumento20 pagineLeukocyte DisordersRaymond MalubayNessuna valutazione finora
- Hodgkin's & NH LymphomaDocumento63 pagineHodgkin's & NH LymphomaHabiba MehmoodNessuna valutazione finora
- Final Year MB CHB Revision Haematology: DR M Drummond Cons Haem, GGH & BocDocumento86 pagineFinal Year MB CHB Revision Haematology: DR M Drummond Cons Haem, GGH & BocShaun TanNessuna valutazione finora
- 4b TUMOR JAR RetikuloendotelialAAADocumento98 pagine4b TUMOR JAR RetikuloendotelialAAARyo RyozNessuna valutazione finora
- Lymphoma CancerDocumento34 pagineLymphoma CancerwasihaiderkNessuna valutazione finora
- Lymph Node CytologyDocumento55 pagineLymph Node CytologyBoy blueNessuna valutazione finora
- RHEUMATOLOGYDocumento121 pagineRHEUMATOLOGYYuni Pratiwi80% (5)
- Leukocytes White Blood CellsDocumento64 pagineLeukocytes White Blood CellsNevin BhunjunNessuna valutazione finora
- Chronic LeukemiaDocumento38 pagineChronic LeukemiaV Lee 'Nozhat'100% (1)
- Kelainan Di Rongga Mulut Karena Gangguan Leukosit (Leukemia)Documento60 pagineKelainan Di Rongga Mulut Karena Gangguan Leukosit (Leukemia)Justin Michal DassNessuna valutazione finora
- Lecture SlidesDocumento86 pagineLecture SlidesJyotsna NigamNessuna valutazione finora
- Acute Leukemia: David Lee, MD, FRCPCDocumento31 pagineAcute Leukemia: David Lee, MD, FRCPCfranzzjosefNessuna valutazione finora
- Lecture 5.16 - LeucaemiaDocumento16 pagineLecture 5.16 - LeucaemiajernsssNessuna valutazione finora
- Chronic Lymphocytic Leukemia (CLL)Documento38 pagineChronic Lymphocytic Leukemia (CLL)Vikkineshwaran Siva Subramaniam100% (2)
- Leukocyte DisordersDocumento55 pagineLeukocyte DisordersSherlyn Yee100% (1)
- Blood Count Interpretation 1Documento49 pagineBlood Count Interpretation 1ripangaNessuna valutazione finora
- Atypical Squamous Cells HPV of FGTDocumento25 pagineAtypical Squamous Cells HPV of FGTNatalia HaikaliNessuna valutazione finora
- WBC Disorders StudentsDocumento81 pagineWBC Disorders Studentskimberly abianNessuna valutazione finora
- One World One People: Jim Rohn, Responding To US Terrorist AttackDocumento67 pagineOne World One People: Jim Rohn, Responding To US Terrorist AttackEko PriyantoNessuna valutazione finora
- Hematopoietic and Lymphoid Systems: - Main Entities - Disorders - Exam Questions and Very ConciseDocumento49 pagineHematopoietic and Lymphoid Systems: - Main Entities - Disorders - Exam Questions and Very ConciseAbbi Yanto ArtNessuna valutazione finora
- Acute Lymphoblastic LeukaemiaDocumento20 pagineAcute Lymphoblastic LeukaemiaPrincewill SeiyefaNessuna valutazione finora
- Back Up Slide ALL SkingDocumento20 pagineBack Up Slide ALL SkingFebry BieluciousNessuna valutazione finora
- Hodgkins Lymphoma by Dr. Anum UsmanDocumento48 pagineHodgkins Lymphoma by Dr. Anum UsmanHumar Haider100% (1)
- Connect Tissue 200002Documento54 pagineConnect Tissue 200002AyeshaNessuna valutazione finora
- Leukaemia & LymphomaDocumento92 pagineLeukaemia & LymphomaSamer FarhanNessuna valutazione finora
- Week 05. Acute LeukemiasDocumento26 pagineWeek 05. Acute LeukemiasAshley ArnoldNessuna valutazione finora
- Hematopathlogy 2Documento87 pagineHematopathlogy 2evansmando12Nessuna valutazione finora
- Hodgkin's LymphomaDocumento106 pagineHodgkin's Lymphomawelly1962Nessuna valutazione finora
- Ug PDFDocumento28 pagineUg PDFSujoita SarkarNessuna valutazione finora
- Lymphoid NeoplasmsDocumento38 pagineLymphoid NeoplasmssaketNessuna valutazione finora
- SleDocumento66 pagineSleNur Liyana Ahmad Zaki100% (1)
- Keganasan HematologiDocumento26 pagineKeganasan HematologiRizzal Selviyana SuhardiNessuna valutazione finora
- Leukemia PresentationDocumento19 pagineLeukemia Presentationayshu4377Nessuna valutazione finora
- Blockxiv Neoplasms Lymphoid 2006Documento54 pagineBlockxiv Neoplasms Lymphoid 2006Ryo RyozNessuna valutazione finora
- Hematology Review: by Felicia Magee Tardy, M.S., MT (Ascp)Documento52 pagineHematology Review: by Felicia Magee Tardy, M.S., MT (Ascp)Adhi TjahyadiNessuna valutazione finora
- Chronic Lymphoid LeukaemiaDocumento23 pagineChronic Lymphoid LeukaemiaAyensuaNessuna valutazione finora
- Lab Diagnosis of Enteric FeverDocumento7 pagineLab Diagnosis of Enteric FeversaketNessuna valutazione finora
- Culture Characteristics of Common OrganismsDocumento5 pagineCulture Characteristics of Common OrganismssaketNessuna valutazione finora
- Lab Diagnosis of Bacillary DysenteryDocumento3 pagineLab Diagnosis of Bacillary Dysenterysaket100% (2)
- Lab Diagnosis of Wound InfectionDocumento3 pagineLab Diagnosis of Wound InfectionsaketNessuna valutazione finora
- Antigens: DR Debasis BiswasDocumento3 pagineAntigens: DR Debasis BiswassaketNessuna valutazione finora
- STR FX Immune SystemDocumento5 pagineSTR FX Immune SystemsaketNessuna valutazione finora
- Immunology An OverviewDocumento4 pagineImmunology An OverviewsaketNessuna valutazione finora
- CardiomyopathyDocumento48 pagineCardiomyopathysaketNessuna valutazione finora
- Normal HematopoesiseDocumento35 pagineNormal HematopoesisesaketNessuna valutazione finora
- Microcytic Hypochromic AnemiasDocumento19 pagineMicrocytic Hypochromic Anemiassaket100% (2)
- Anemia ApproachDocumento50 pagineAnemia ApproachsaketNessuna valutazione finora
- Acquired Hemolytic AnemiaDocumento24 pagineAcquired Hemolytic AnemiasaketNessuna valutazione finora
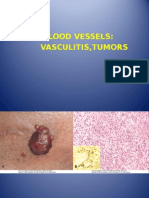
- BV Vasculitis TumorsDocumento11 pagineBV Vasculitis TumorssaketNessuna valutazione finora
- AtherosclerosisDocumento22 pagineAtherosclerosissaketNessuna valutazione finora
- Congenital Heart DiseaseDocumento47 pagineCongenital Heart DiseasesaketNessuna valutazione finora
- Coagulation DisordersDocumento35 pagineCoagulation DisorderssaketNessuna valutazione finora
- Hemostatic DisordersDocumento57 pagineHemostatic DisorderssaketNessuna valutazione finora
- Lymphoid NeoplasmsDocumento38 pagineLymphoid NeoplasmssaketNessuna valutazione finora
- Myeloproliferative NeoplasmsDocumento59 pagineMyeloproliferative NeoplasmssaketNessuna valutazione finora
- WBC DisordersDocumento60 pagineWBC DisorderssaketNessuna valutazione finora
- v4n4 PDFDocumento185 paginev4n4 PDFJorge RodriguezNessuna valutazione finora
- DBT BET Question Paper 2009 With Answer KeyDocumento22 pagineDBT BET Question Paper 2009 With Answer KeyAbhay Kumar100% (3)
- Lower Immune System ResponseDocumento25 pagineLower Immune System ResponsemakajeNessuna valutazione finora
- Monoclonal AntibodiesDocumento27 pagineMonoclonal AntibodiesFrannie NillamaNessuna valutazione finora
- LES y Enf CardiovascularDocumento15 pagineLES y Enf CardiovascularSMIBA MedicinaNessuna valutazione finora
- Drugs Acting On The Immune System: Retchel-Elly D. Dapli-AnDocumento60 pagineDrugs Acting On The Immune System: Retchel-Elly D. Dapli-AnJoshua MendozaNessuna valutazione finora
- Immunology 1700s: Immunology and Serology Terminologies and Historical BackgroundDocumento3 pagineImmunology 1700s: Immunology and Serology Terminologies and Historical BackgroundLyka ReyesNessuna valutazione finora
- HHS Public Access: B Cell Targeted Therapies in Autoimmune DiseaseDocumento15 pagineHHS Public Access: B Cell Targeted Therapies in Autoimmune DiseaseLestiNessuna valutazione finora
- Bio ProjectDocumento25 pagineBio Projectlipi galotNessuna valutazione finora
- The Immune System Report OutlineDocumento3 pagineThe Immune System Report Outlinemattlight07Nessuna valutazione finora
- PG SyllabusDocumento328 paginePG SyllabusHishar Mirsam100% (1)
- Clinical Manifestation of Oral TuberculosisDocumento6 pagineClinical Manifestation of Oral TuberculosisSasa AprilaNessuna valutazione finora
- IBD Briggs Beta7Documento27 pagineIBD Briggs Beta7Amit Yadav100% (4)
- Autoimmune Hemolytic AnaemiaDocumento32 pagineAutoimmune Hemolytic AnaemiaJohn VinithNessuna valutazione finora
- Role of Neutrophils in Periodontal DiseaseDocumento65 pagineRole of Neutrophils in Periodontal DiseaseGaurav Phaphriya40% (5)
- (Current Cancer Research) Ian Magrath (Auth.), Erle S. Robertson (Eds.) - Burkitt's Lymphoma-Springer-Verlag New York (2013) PDFDocumento333 pagine(Current Cancer Research) Ian Magrath (Auth.), Erle S. Robertson (Eds.) - Burkitt's Lymphoma-Springer-Verlag New York (2013) PDFΑννα ΙωαννουNessuna valutazione finora
- Carte SemioDocumento279 pagineCarte SemioJoão Vitor LacerdaNessuna valutazione finora
- Aids To Health - Important Qs - Important Questions - ICSEDocumento3 pagineAids To Health - Important Qs - Important Questions - ICSEsujata duttaNessuna valutazione finora
- Topics List - First AID 2019Documento28 pagineTopics List - First AID 2019saraNessuna valutazione finora
- Microbial Triggers in Autoimmunity, Severe Allergy, and AutoallergyDocumento16 pagineMicrobial Triggers in Autoimmunity, Severe Allergy, and AutoallergyMystero RasicoNessuna valutazione finora
- BSC Micorbiology CUCBSSDocumento35 pagineBSC Micorbiology CUCBSSJaseena AlNessuna valutazione finora
- BSC Immunology Course Sylibus - Updated 1st Sem. 2022-2023Documento3 pagineBSC Immunology Course Sylibus - Updated 1st Sem. 2022-2023Basma MohamedNessuna valutazione finora
- Psoriasis Types Causes Medication I To 13Documento189 paginePsoriasis Types Causes Medication I To 13jimdioNessuna valutazione finora
- Endocrinology and IridologyDocumento136 pagineEndocrinology and Iridologygelongnavarro100% (3)
- Biology Investigatory Project Viral DiseasesDocumento16 pagineBiology Investigatory Project Viral DiseasesAman MujeebNessuna valutazione finora
- Cell Recognition and The Immune SystemDocumento23 pagineCell Recognition and The Immune SystemSaeed Abdulhadi100% (1)
- Pratiwi S Gunawan, BDS., DDS., MDSC, PHDDocumento53 paginePratiwi S Gunawan, BDS., DDS., MDSC, PHDBima Ewando KabanNessuna valutazione finora
- Budwig Cancer GuideDocumento110 pagineBudwig Cancer GuideDejan Velkovski100% (2)
- Spittler Et Al. - 1995 - Influence of Glutamine On The Phenotype and FunctiDocumento6 pagineSpittler Et Al. - 1995 - Influence of Glutamine On The Phenotype and FunctiMATHILDE MAGRONessuna valutazione finora
- Neutrophils in Pancreatic Cancer ProgressionDocumento103 pagineNeutrophils in Pancreatic Cancer ProgressionShahid ShaikhNessuna valutazione finora