Potrebbero piacerti anche
- TuberculosisDocumento58 pagineTuberculosishemaanandhyNessuna valutazione finora
- Bronchitis Acute Brochitis: DefinitionDocumento7 pagineBronchitis Acute Brochitis: DefinitionhemaanandhyNessuna valutazione finora
- Chest PhysiotherapyDocumento16 pagineChest Physiotherapyhemaanandhy75% (4)
- Bronchitis Acute Brochitis: DefinitionDocumento7 pagineBronchitis Acute Brochitis: DefinitionhemaanandhyNessuna valutazione finora
- HypertensionDocumento4 pagineHypertensionhemaanandhyNessuna valutazione finora
- Status Asthmaticus: Severe Persistent AsthmaDocumento2 pagineStatus Asthmaticus: Severe Persistent Asthmahemaanandhy0% (1)
- RhinitisDocumento30 pagineRhinitishemaanandhyNessuna valutazione finora
- Chronic Obstructive Pulmonary Disease (Copd)Documento16 pagineChronic Obstructive Pulmonary Disease (Copd)hemaanandhyNessuna valutazione finora
- TB Management EnglishDocumento1 paginaTB Management EnglishhemaanandhyNessuna valutazione finora
- Chronic Obstructive Pulmonary Disease (Copd)Documento16 pagineChronic Obstructive Pulmonary Disease (Copd)hemaanandhyNessuna valutazione finora
- BronchitisDocumento18 pagineBronchitishemaanandhyNessuna valutazione finora
- Pneumonia: DefinitionDocumento5 paginePneumonia: DefinitionhemaanandhyNessuna valutazione finora
- Motor TestingDocumento57 pagineMotor TestinghemaanandhyNessuna valutazione finora
- Un ConsiousnessDocumento25 pagineUn Consiousnesshemaanandhy100% (1)
- Atherosclerosis DefenitionDocumento3 pagineAtherosclerosis DefenitionhemaanandhyNessuna valutazione finora
- FWPDocumento37 pagineFWPhemaanandhyNessuna valutazione finora
- Cerebro Vascular Accident (Cva)Documento3 pagineCerebro Vascular Accident (Cva)hemaanandhyNessuna valutazione finora
- Stroke SriDocumento34 pagineStroke SrihemaanandhyNessuna valutazione finora
- Environmental Sanitation 473Documento36 pagineEnvironmental Sanitation 473powerpufflomu100% (1)
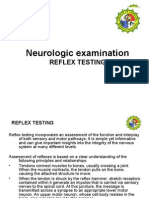
- Reflex TestingDocumento44 pagineReflex Testingsarguss14100% (7)
- Unit Plan ON Medical Surgical Nursing: M.SC Nursing I YearDocumento7 pagineUnit Plan ON Medical Surgical Nursing: M.SC Nursing I YearhemaanandhyNessuna valutazione finora
- Sensory ExamDocumento24 pagineSensory Examsarguss14100% (2)
- Crtical CareDocumento44 pagineCrtical CarehemaanandhyNessuna valutazione finora
- Scope of EpidemiologyDocumento29 pagineScope of Epidemiologyhemaanandhy71% (7)
- EXTERNAL EAR DISORDERS AND DEFORMITIESDocumento48 pagineEXTERNAL EAR DISORDERS AND DEFORMITIEShemaanandhyNessuna valutazione finora
- EpidemiologyDocumento50 pagineEpidemiologyhemaanandhyNessuna valutazione finora
- Community IDocumento13 pagineCommunity IhemaanandhyNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Case Study On Maruti 800Documento4 pagineCase Study On Maruti 800Nizar MesaniNessuna valutazione finora
- Applied Physics Mini Launcher Lab ReportDocumento12 pagineApplied Physics Mini Launcher Lab ReportTalharashid RamzanNessuna valutazione finora
- ECE 4400 Performance Analysis Local Computer Networks HomeworkDocumento2 pagineECE 4400 Performance Analysis Local Computer Networks HomeworkNguyen Phi HungNessuna valutazione finora
- Clinical behavior analysis and RFT: Conceptualizing psychopathology and its treatmentDocumento28 pagineClinical behavior analysis and RFT: Conceptualizing psychopathology and its treatmentAnne de AndradeNessuna valutazione finora
- HYBT Series: Assembling Terminal BlockDocumento8 pagineHYBT Series: Assembling Terminal Blockanon_670965762Nessuna valutazione finora
- Philosophy of Disciple Making PaperDocumento5 paginePhilosophy of Disciple Making Paperapi-665038631Nessuna valutazione finora
- 1HMEE5013 Exam Q JAN2017 S14Documento5 pagine1HMEE5013 Exam Q JAN2017 S14kumar6125100% (1)
- 341SAM Ethical Leadership - Alibaba FinalDocumento16 pagine341SAM Ethical Leadership - Alibaba FinalPhoebe CaoNessuna valutazione finora
- Community Development A Critical Approach PDFDocumento2 pagineCommunity Development A Critical Approach PDFNatasha50% (2)
- Quantitative Aptitude-More Exercise Questions Updated On Jul 2019Documento4 pagineQuantitative Aptitude-More Exercise Questions Updated On Jul 2019SANAMGI BHAVYANessuna valutazione finora
- Adjutant-Introuvable BASIC VERSIONDocumento7 pagineAdjutant-Introuvable BASIC VERSIONfurrypdfNessuna valutazione finora
- Hmdu - EnglishDocumento20 pagineHmdu - EnglishAbdulaziz SeikoNessuna valutazione finora
- Tender Evaluation Template GuideDocumento15 pagineTender Evaluation Template GuideKhalid NaeemNessuna valutazione finora
- 3 - 6consctructing Probability Distributions CG A - 4 - 6 Lesson 2Documento24 pagine3 - 6consctructing Probability Distributions CG A - 4 - 6 Lesson 2CHARLYN JOY SUMALINOGNessuna valutazione finora
- Ips 350:400:450:500:600 07:05 PDFDocumento124 pagineIps 350:400:450:500:600 07:05 PDFRandall PettersonNessuna valutazione finora
- 1 CAT O&M Manual G3500 Engine 0Documento126 pagine1 CAT O&M Manual G3500 Engine 0Hassan100% (1)
- BRKSPG-2904-2904 - Cisco Live Session - v2-CL PDFDocumento182 pagineBRKSPG-2904-2904 - Cisco Live Session - v2-CL PDFMohamed SamirNessuna valutazione finora
- Pressing and Finishing (Latest)Documento8 paginePressing and Finishing (Latest)Imran TexNessuna valutazione finora
- Ragavendhar Seeks Entry Software JobDocumento2 pagineRagavendhar Seeks Entry Software JobfferferfNessuna valutazione finora
- Appraisal Sample PDFDocumento22 pagineAppraisal Sample PDFkiruthikaNessuna valutazione finora
- Westford University College readies flagship campus with new programsDocumento20 pagineWestford University College readies flagship campus with new programsSaju JanardhananNessuna valutazione finora
- Chapter 1 Critical Thin...Documento7 pagineChapter 1 Critical Thin...sameh06Nessuna valutazione finora
- Mega Goal 4Documento52 pagineMega Goal 4mahgoubkamel0% (1)
- Open MPDocumento30 pagineOpen MPmacngocthanNessuna valutazione finora
- FAI - Assignment Sheet (Both Assignments)Documento5 pagineFAI - Assignment Sheet (Both Assignments)Wilson WongNessuna valutazione finora
- Math 2 Curriculum GuideDocumento19 pagineMath 2 Curriculum GuideMichelle Villanueva Jalando-onNessuna valutazione finora
- MAN 2 Model Medan Introduction to School Environment ReportDocumento45 pagineMAN 2 Model Medan Introduction to School Environment ReportdindaNessuna valutazione finora
- ccpc15 Supportive and Preventive WorkbookDocumento30 pagineccpc15 Supportive and Preventive WorkbookJeremy HamptonNessuna valutazione finora
- MEC332-MA 3rd Sem - Development EconomicsDocumento9 pagineMEC332-MA 3rd Sem - Development EconomicsRITUPARNA KASHYAP 2239239Nessuna valutazione finora
- Transistor Amplifier Operating ParametersDocumento21 pagineTransistor Amplifier Operating ParametersReddyvari VenugopalNessuna valutazione finora