Potrebbero piacerti anche
- Introduction To UrologyDocumento48 pagineIntroduction To UrologyvaiyenNessuna valutazione finora
- Expert Guide to Psoas Major Function and Body MechanicsDocumento15 pagineExpert Guide to Psoas Major Function and Body MechanicstokionasNessuna valutazione finora
- Somanabolic Weight TrainingDocumento70 pagineSomanabolic Weight TrainingNorma A Levasseur50% (2)
- Scanning Technique of KidneysDocumento103 pagineScanning Technique of KidneysPhuntsho OngmoNessuna valutazione finora
- Renal Ultrasound: Diana Pancu, MDDocumento76 pagineRenal Ultrasound: Diana Pancu, MDReza Angga PratamaNessuna valutazione finora
- HydronephrosisDocumento43 pagineHydronephrosisjessyNessuna valutazione finora
- Imaging in Genitourinary SystemDocumento77 pagineImaging in Genitourinary SystemIrvan R. Loho100% (1)
- Men's Health Total Body Muscle PlanDocumento44 pagineMen's Health Total Body Muscle PlanJaydev RavalNessuna valutazione finora
- Pelvic Dysfunction in Men: Diagnosis and Treatment of Male Incontinence and Erectile DysfunctionDa EverandPelvic Dysfunction in Men: Diagnosis and Treatment of Male Incontinence and Erectile DysfunctionNessuna valutazione finora
- Urolithiasis SeminarDocumento50 pagineUrolithiasis SeminarSiddharth GuptaNessuna valutazione finora
- HematuriaDocumento86 pagineHematuriaMohamad Arif MustaphaNessuna valutazione finora
- The Ventricular System of The BrainDocumento35 pagineThe Ventricular System of The BrainBaguma MichaelNessuna valutazione finora
- Renal and Ureteric Calculi: Causes, Types, Diagnosis and TreatmentDocumento27 pagineRenal and Ureteric Calculi: Causes, Types, Diagnosis and TreatmentJaymalya100% (4)
- Imaging in Genitourinary System - 17 Agustus 2013 - by Robby HermawanDocumento80 pagineImaging in Genitourinary System - 17 Agustus 2013 - by Robby HermawanFitria Dewi LestariNessuna valutazione finora
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesDa EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesValutazione: 5 su 5 stelle5/5 (2)
- Introduction Urinary SystemDocumento19 pagineIntroduction Urinary SystemKatherine Anne ReyesNessuna valutazione finora
- Pediatric Imaging Cases: Mysteries Solved with RadiologyDocumento82 paginePediatric Imaging Cases: Mysteries Solved with Radiologyabakferro0% (1)
- Uterovaginal ProlapseDocumento52 pagineUterovaginal ProlapseAmeera K Khan75% (4)
- Benign Prostatic HyperplasiaDocumento36 pagineBenign Prostatic Hyperplasiamomodou s jallowNessuna valutazione finora
- USG of Normal Musculoskeletal StructuresDocumento7 pagineUSG of Normal Musculoskeletal StructuresDhisa Zainita HabsariNessuna valutazione finora
- Lab Exercise No. 5: X-Ray Identification Activity: Name: Rocel Marie D. Lopez Section: BSN 1105Documento11 pagineLab Exercise No. 5: X-Ray Identification Activity: Name: Rocel Marie D. Lopez Section: BSN 1105Rocel Marie Lopez100% (1)
- Clinical Examination of Genitourinary SystemDocumento43 pagineClinical Examination of Genitourinary SystemKeamina .aNessuna valutazione finora
- Detailed Lesson PlanDocumento49 pagineDetailed Lesson PlanNaisy MagalonaNessuna valutazione finora
- Gorilla WorkoutDocumento4 pagineGorilla WorkoutKishoreVancheeshwaranNessuna valutazione finora
- The Perfect Pancreatitis Diet Cookbook; The Complete Nutrition Guide To Managing And Healing Pancreatitis With Delectable And Nourishing Recipes;Da EverandThe Perfect Pancreatitis Diet Cookbook; The Complete Nutrition Guide To Managing And Healing Pancreatitis With Delectable And Nourishing Recipes;Nessuna valutazione finora
- Urinary Tract Disorders, PowerpointDocumento63 pagineUrinary Tract Disorders, Powerpointmutia mutia100% (4)
- OTR ReviewDocumento64 pagineOTR Reviewkjykiki1986100% (6)
- Basics of Urology: Hematuria, Pain, LUTSDocumento29 pagineBasics of Urology: Hematuria, Pain, LUTSgozali189 biringNessuna valutazione finora
- Imaging in Genitourinary SystemDocumento36 pagineImaging in Genitourinary SystemAlkaustariyah LubisNessuna valutazione finora
- Imaging of The Genito Urinary TractDocumento56 pagineImaging of The Genito Urinary TractAharauka ChiedozieNessuna valutazione finora
- Imaging Tractus UrinaryDocumento94 pagineImaging Tractus UrinaryJuan Ortega PutraNessuna valutazione finora
- The Urinary TractDocumento44 pagineThe Urinary TractMarina RotaruNessuna valutazione finora
- Imaging Modalities of the Genitourinary SystemDocumento59 pagineImaging Modalities of the Genitourinary SystemMUBIRU SAMUEL EDWARDNessuna valutazione finora
- History Taking and Physical Examination in Urologic PatientsDocumento25 pagineHistory Taking and Physical Examination in Urologic PatientsAdebisiNessuna valutazione finora
- Kidney, Ureter, Bladder and Prostate Pain SyndromesDocumento69 pagineKidney, Ureter, Bladder and Prostate Pain SyndromesKaram SaadNessuna valutazione finora
- 3 Obat Sedasi Dan Analgesia-Prof Munar - LubisDocumento93 pagine3 Obat Sedasi Dan Analgesia-Prof Munar - LubisFahmi NurNessuna valutazione finora
- Urinary System RadiographyDocumento32 pagineUrinary System RadiographyVivek ChaudharyNessuna valutazione finora
- Imaging GU Tract Modalities Guide - IVU, Cystography, UrethrographyDocumento86 pagineImaging GU Tract Modalities Guide - IVU, Cystography, UrethrographyNor AinaNessuna valutazione finora
- Gangguan Sistem Perkemihan: DR A. Yuda Handaya, SPB, Finacs, FmasDocumento132 pagineGangguan Sistem Perkemihan: DR A. Yuda Handaya, SPB, Finacs, FmasRobby Wiranata WijayaNessuna valutazione finora
- 10 - Urological DiordersDocumento47 pagine10 - Urological Diordersgozali189 biringNessuna valutazione finora
- Urinary Tract ImagingDocumento39 pagineUrinary Tract ImagingYuda FhunkshyangNessuna valutazione finora
- General Anatomu UrologyDocumento60 pagineGeneral Anatomu UrologyAllan ManiNessuna valutazione finora
- Imaging of The Genitourinary Tract: Mashuri, DR.,SP - Rad.,M.KesDocumento90 pagineImaging of The Genitourinary Tract: Mashuri, DR.,SP - Rad.,M.KesmirzasullivanNessuna valutazione finora
- URINARY SYSTEM ANATOMY & CONTRAST STUDIESDocumento15 pagineURINARY SYSTEM ANATOMY & CONTRAST STUDIESRhahima SyafrilNessuna valutazione finora
- Investigations of The Urinary TractDocumento26 pagineInvestigations of The Urinary TractOnkar SinghNessuna valutazione finora
- KDI306 - L34 Tramed BOF - IVUDocumento93 pagineKDI306 - L34 Tramed BOF - IVUYodi SoebadiNessuna valutazione finora
- Chapter 57 Introduction To The Urinary SystemDocumento24 pagineChapter 57 Introduction To The Urinary SystemtikkimarshallNessuna valutazione finora
- Sites: - Ureteric CalculiDocumento16 pagineSites: - Ureteric CalculiBersisa chalchisaNessuna valutazione finora
- Acute Intestinal ObstructionDocumento38 pagineAcute Intestinal ObstructiondinahzrNessuna valutazione finora
- Renal SurgeryDocumento62 pagineRenal Surgeryalvin salvationNessuna valutazione finora
- b9 PKM 2 Urinary Retention Dr. Christian Ronald Tanggo Sp.uDocumento63 pagineb9 PKM 2 Urinary Retention Dr. Christian Ronald Tanggo Sp.uDaud ParluhutanNessuna valutazione finora
- 3-Basic Concepts in Diagnostic ImagingDocumento60 pagine3-Basic Concepts in Diagnostic ImagingAmd SolihinNessuna valutazione finora
- Examination and Investigation of The Urogenital System For GUUDocumento40 pagineExamination and Investigation of The Urogenital System For GUUJake MillerNessuna valutazione finora
- Lecture Notes On Medical Nursing IiiDocumento614 pagineLecture Notes On Medical Nursing IiiAnim Richard DuoduNessuna valutazione finora
- Presentation Liver UltrasoundDocumento21 paginePresentation Liver UltrasoundDanielle FosterNessuna valutazione finora
- Urinary RetentionDocumento64 pagineUrinary RetentionAntonioIndraTNessuna valutazione finora
- Prostae UroDocumento43 pagineProstae UroShidevNessuna valutazione finora
- Lecture 2 (Prostatitis)Documento43 pagineLecture 2 (Prostatitis)Rian Permana PNessuna valutazione finora
- Abdominal anatomy assessment: Key techniques for inspection, auscultation, percussion and palpationDocumento55 pagineAbdominal anatomy assessment: Key techniques for inspection, auscultation, percussion and palpationJackie BringhurstNessuna valutazione finora
- Intestinal ObstructionDocumento27 pagineIntestinal ObstructionAna AvilaNessuna valutazione finora
- Intestinal ObstructionDocumento12 pagineIntestinal ObstructionNurul Nurnita100% (1)
- Radiology of Hepatobiliary System, Pancreas and SpleenDocumento136 pagineRadiology of Hepatobiliary System, Pancreas and SpleenShubham TanwarNessuna valutazione finora
- Ivp Intravenous PyelographyDocumento16 pagineIvp Intravenous PyelographyLuisa ManaloNessuna valutazione finora
- Urology Basics: Hematuria GuideDocumento171 pagineUrology Basics: Hematuria GuideDr Anais AsimNessuna valutazione finora
- Abdominal SonographyDocumento6 pagineAbdominal SonographyRio FutabaNessuna valutazione finora
- Renal Stones: Causes, Symptoms & TreatmentDocumento15 pagineRenal Stones: Causes, Symptoms & TreatmentGabrielle Frances FernandezNessuna valutazione finora
- Acute Urinary Retention: Ronald TanggoDocumento63 pagineAcute Urinary Retention: Ronald TanggoKalista ApriyaniNessuna valutazione finora
- The Role of The Laboratory in Renal Diseases-2015-16Documento67 pagineThe Role of The Laboratory in Renal Diseases-2015-16wiamNessuna valutazione finora
- Batu Saluran Kemih: Dr. Elli Arsita, SPPD Departemen Ilmu Penyakit Dalam FK UkridaDocumento22 pagineBatu Saluran Kemih: Dr. Elli Arsita, SPPD Departemen Ilmu Penyakit Dalam FK UkridaJoshua DjohanNessuna valutazione finora
- DafpusDocumento8 pagineDafpusNaja HasnandaNessuna valutazione finora
- As HyaluronatvaginitisatropiebmDocumento6 pagineAs HyaluronatvaginitisatropiebmNaja HasnandaNessuna valutazione finora
- Metabsyndrome SirosisDocumento7 pagineMetabsyndrome SirosisNaja HasnandaNessuna valutazione finora
- Rapid Test HivDocumento14 pagineRapid Test HivNaja HasnandaNessuna valutazione finora
- Evaluation and Management of Herpes Zoster OphthalmicusDocumento8 pagineEvaluation and Management of Herpes Zoster OphthalmicusYoser ThamtonoNessuna valutazione finora
- Evaluasi Diare KronikDocumento8 pagineEvaluasi Diare KronikNaja HasnandaNessuna valutazione finora
- Ebm NSCLCDocumento8 pagineEbm NSCLCNaja HasnandaNessuna valutazione finora
- Medically Indicated LateDocumento3 pagineMedically Indicated LateNaja HasnandaNessuna valutazione finora
- EBM DiagnosisDocumento8 pagineEBM DiagnosisNaja HasnandaNessuna valutazione finora
- Chronik Diare Tidak BerdarahDocumento7 pagineChronik Diare Tidak BerdarahNaja HasnandaNessuna valutazione finora
- PF PulmoDocumento5 paginePF PulmoNaja Hasnanda100% (1)
- Distinguishing Tuberculosis and Crohn's Disease in Developing Countries: How Certain Can You Be of The Diagnosis?Documento5 pagineDistinguishing Tuberculosis and Crohn's Disease in Developing Countries: How Certain Can You Be of The Diagnosis?Naja HasnandaNessuna valutazione finora
- Esofageal CancerDocumento3 pagineEsofageal CancerNaja HasnandaNessuna valutazione finora
- Ebm NSCLCDocumento8 pagineEbm NSCLCNaja HasnandaNessuna valutazione finora
- Risk Epilepsy TraumaDocumento7 pagineRisk Epilepsy TraumaNaja HasnandaNessuna valutazione finora
- Consensus Guidelines On The Management of Epilepsy 2010Documento94 pagineConsensus Guidelines On The Management of Epilepsy 2010alivestyledNessuna valutazione finora
- EBM DiagnosisDocumento8 pagineEBM DiagnosisNaja HasnandaNessuna valutazione finora
- Jurnal Ebm NSCLCDocumento10 pagineJurnal Ebm NSCLCNaja HasnandaNessuna valutazione finora
- Hepatocellullar Carcinoma Pathogenesis JournalDocumento20 pagineHepatocellullar Carcinoma Pathogenesis JournalNaja HasnandaNessuna valutazione finora
- 12-Week Full Body Workout SplitDocumento4 pagine12-Week Full Body Workout SplitDakota SheppardNessuna valutazione finora
- DUR - Fracture of The Shaft Radius and UlnaDocumento55 pagineDUR - Fracture of The Shaft Radius and UlnaM. Abdurrahman Al-HaraaniNessuna valutazione finora
- 22 Respiratory SystemDocumento99 pagine22 Respiratory SystemvanderphysNessuna valutazione finora
- Endocrine Glands - 1st - ChapterDocumento12 pagineEndocrine Glands - 1st - Chaptervarun kumarNessuna valutazione finora
- Miniscrew-Assisted Mandibular Molar Protraction: A Case ReportDocumento6 pagineMiniscrew-Assisted Mandibular Molar Protraction: A Case ReportAdvanced Research PublicationsNessuna valutazione finora
- Lecture 7 Anterior & Posterior Crossbites (6 Per Page) (Compatibility Mode)Documento14 pagineLecture 7 Anterior & Posterior Crossbites (6 Per Page) (Compatibility Mode)dent in dentistNessuna valutazione finora
- Nasopharyngeal Angiofibroma Treatment OptionsDocumento51 pagineNasopharyngeal Angiofibroma Treatment OptionsMiranda Yudhi CyubidubiduuNessuna valutazione finora
- The Nervous System & Our Brain PowerPoint - Krishna ShilDocumento21 pagineThe Nervous System & Our Brain PowerPoint - Krishna ShilKrishna ShilNessuna valutazione finora
- Cranial NervesDocumento90 pagineCranial NervesGaVee AgranNessuna valutazione finora
- Catio Lift Eye TreamentDocumento2 pagineCatio Lift Eye TreamentNazihCosmeticsNessuna valutazione finora
- Terumo Europe Cardiovascular Systems 2009 Terumo Europe Cardiovascular SystemsDocumento142 pagineTerumo Europe Cardiovascular Systems 2009 Terumo Europe Cardiovascular SystemsManigandan DhamodhiranNessuna valutazione finora
- 10,11-Arterial Blood Pressure & Its Regulation Team441Documento51 pagine10,11-Arterial Blood Pressure & Its Regulation Team441saran kNessuna valutazione finora
- Graves' Disease OverviewDocumento1 paginaGraves' Disease OverviewMichael PutraNessuna valutazione finora
- 1.1 Surface Anatomy and Surface Landmarks For Thoracic SurgeryDocumento13 pagine1.1 Surface Anatomy and Surface Landmarks For Thoracic SurgeryResidentes CirugíaNessuna valutazione finora
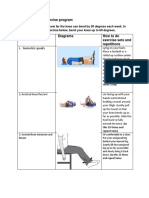
- Home Exercise ProgramDocumento3 pagineHome Exercise ProgramKgabo MadubanyaNessuna valutazione finora
- Local anaesthesia techniques for dental proceduresDocumento26 pagineLocal anaesthesia techniques for dental proceduresGeorge MKNessuna valutazione finora
- NIKE-The Program DefenceDocumento20 pagineNIKE-The Program DefenceCharlotteEngNessuna valutazione finora
- Worksheet BiologyDocumento2 pagineWorksheet BiologyRidham JainNessuna valutazione finora
- Classification of Partially Edentulous ArchesDocumento27 pagineClassification of Partially Edentulous ArchesBharti DuaNessuna valutazione finora
- HLC ProceduresDocumento13 pagineHLC ProceduresMhel MGNessuna valutazione finora
- Reviewer Science For Grade 9 StudentsDocumento29 pagineReviewer Science For Grade 9 StudentsevanescentNessuna valutazione finora