Potrebbero piacerti anche
- 2020-11-25 New Enzyplex - Prof. Marcel - The Role of Digestive Enzymes Supplement in FunctionalDocumento54 pagine2020-11-25 New Enzyplex - Prof. Marcel - The Role of Digestive Enzymes Supplement in Functionalgraha internaNessuna valutazione finora
- Thyroid Function TestDocumento21 pagineThyroid Function TestPat JacintoNessuna valutazione finora
- Gastrointestinal DrugsDocumento23 pagineGastrointestinal Drugsarifudin100% (1)
- Antiemetics: Dr. Bikram TewariDocumento31 pagineAntiemetics: Dr. Bikram TewariRajkamal SarmaNessuna valutazione finora
- Adrenal Gland DisordersDocumento7 pagineAdrenal Gland Disorderscn351073Nessuna valutazione finora
- Pharmacotherapy of DMDocumento23 paginePharmacotherapy of DMsalinaNessuna valutazione finora
- HypothyridismDocumento18 pagineHypothyridismanuu1404Nessuna valutazione finora
- Insulin PharmDocumento21 pagineInsulin PharmMeredith Barb0% (1)
- Pain ManagementDocumento39 paginePain Managementsteven saputra100% (1)
- GastroenteritisDocumento27 pagineGastroenteritisJhoanna Jhoi Alves VarillaNessuna valutazione finora
- Drugs Interaction1Documento13 pagineDrugs Interaction1Akshay MandhotraNessuna valutazione finora
- Organophosphate PoisoningDocumento19 pagineOrganophosphate PoisoningapokawNessuna valutazione finora
- Emergency Drugs: (A Drug Study)Documento13 pagineEmergency Drugs: (A Drug Study)Marichu BajadoNessuna valutazione finora
- Antiparkinsons DrugsDocumento19 pagineAntiparkinsons Drugs39 Nayan BhagatNessuna valutazione finora
- Nootropil: Qualitative and Quantitative CompositionDocumento12 pagineNootropil: Qualitative and Quantitative CompositionMuhammad TalhaNessuna valutazione finora
- Drugs in PregnancyDocumento33 pagineDrugs in PregnancyserbalexNessuna valutazione finora
- Anticholinergic DrugsDocumento19 pagineAnticholinergic DrugseashshankarNessuna valutazione finora
- Cushing - AddisonDocumento27 pagineCushing - AddisonMelissa-Andreea Ardeleanu Carvajal OsorioNessuna valutazione finora
- Clinical Pharmacy Lab - Quiz Part 2Documento4 pagineClinical Pharmacy Lab - Quiz Part 2Aassh DcmbrNessuna valutazione finora
- Pharmacotherapy of Diabetes Mellitus: Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaDocumento42 paginePharmacotherapy of Diabetes Mellitus: Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaEya Prepti SerraNessuna valutazione finora
- CorticosteroidsDocumento8 pagineCorticosteroidsAkuMrW100% (1)
- ChemotherapyDocumento35 pagineChemotherapynikhl saulNessuna valutazione finora
- Anti Epileptic DrugsDocumento6 pagineAnti Epileptic DrugsFaria Islam JuhiNessuna valutazione finora
- Pancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyDocumento69 paginePancreatic Hormone & Antidiabetic Drugs: Renato I. Dalmacio, RPH Pharmacology 414 College of PharmacyRalf EmoteroNessuna valutazione finora
- Corticosteroids 2 of 2Documento33 pagineCorticosteroids 2 of 2VLDsNessuna valutazione finora
- Coronary Heart DiseaseDocumento11 pagineCoronary Heart DiseaseZaryna TohNessuna valutazione finora
- Anatomy and Physiology of The ColonDocumento3 pagineAnatomy and Physiology of The ColonMenchie Vivas-AlotNessuna valutazione finora
- Drug Used in Skin and Mucus MembraneDocumento35 pagineDrug Used in Skin and Mucus MembraneMamta Yadav100% (1)
- Drug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineDocumento21 pagineDrug Induced Hepatitis: Dr.M.Sharmila Assistant Professor M7 (Prof CR Unit) Institute of Internal MedicineAtakan Yeşil100% (1)
- Hematinic AgentsDocumento89 pagineHematinic AgentsHussain Rizvi50% (2)
- MM MM MM MM MMM MMMMM M MM M MMMM MMMMM MMM MM MMM MM!M M!"M#MM MM M $M M %MMM MM "M "MM M MMM MDocumento9 pagineMM MM MM MM MMM MMMMM M MM M MMMM MMMMM MMM MM MMM MM!M M!"M#MM MM M $M M %MMM MM "M "MM M MMM M배기숭Nessuna valutazione finora
- NCM116 Addison DiseaseDocumento20 pagineNCM116 Addison DiseaseSofia MikaelaNessuna valutazione finora
- Cancer ChemotherapyDocumento28 pagineCancer ChemotherapyFidelis LovelyNessuna valutazione finora
- Cushing DiseaseDocumento24 pagineCushing DiseaseSuci AlimaNessuna valutazione finora
- Concept of Shatkriyakala As Mentioned in Sushruta SamhitaDocumento3 pagineConcept of Shatkriyakala As Mentioned in Sushruta SamhitaAdvanced Research PublicationsNessuna valutazione finora
- Routes of Drug AdministrationDocumento37 pagineRoutes of Drug Administrationxq qxNessuna valutazione finora
- Acute Renal Failure & Chronic Renal FailureDocumento38 pagineAcute Renal Failure & Chronic Renal FailureArti GondNessuna valutazione finora
- Serratiopeptidase Is An Enzyme Having AntiDocumento12 pagineSerratiopeptidase Is An Enzyme Having Antidracula386Nessuna valutazione finora
- Pharmacology Renal DiureticsDocumento24 paginePharmacology Renal Diureticskpsuan100% (1)
- 50 One or Two Words OnlyDocumento5 pagine50 One or Two Words OnlyFan EliNessuna valutazione finora
- Thyroid Crisis... FinalDocumento53 pagineThyroid Crisis... FinalYhanaAdarneNessuna valutazione finora
- Adrenocortical HyperfunctionDocumento132 pagineAdrenocortical Hyperfunctionshobharamkrishna100% (2)
- Peptic Ulcer Drugs and Pharmcotherapy - DrdhritiDocumento60 paginePeptic Ulcer Drugs and Pharmcotherapy - Drdhritidbrahma100% (2)
- Zollinger Ellis Wps OfficeDocumento15 pagineZollinger Ellis Wps OfficeAbhash MishraNessuna valutazione finora
- Mesalazine: Mesalazine (INN, BAN), Also Known As Mesalamine (USAN) or 5-Aminosalicylic AcidDocumento4 pagineMesalazine: Mesalazine (INN, BAN), Also Known As Mesalamine (USAN) or 5-Aminosalicylic AcidAnkan PalNessuna valutazione finora
- C. Anti-Hypertensive Drugs.Documento10 pagineC. Anti-Hypertensive Drugs.Nabeel AsifNessuna valutazione finora
- Diabetes Mellitus: Nhamier M. Jikiri, RN, MD, FPCP Internal MedicineDocumento27 pagineDiabetes Mellitus: Nhamier M. Jikiri, RN, MD, FPCP Internal MedicineNursidar Pascual MukattilNessuna valutazione finora
- Peptic UlcerDocumento115 paginePeptic Ulcerjeenath justin doss100% (2)
- Acute GlomerulonephritisDocumento21 pagineAcute Glomerulonephritisbrinda johnNessuna valutazione finora
- Anti - Cancer Drugs 1Documento80 pagineAnti - Cancer Drugs 1Rajkamal Sarma100% (1)
- Guidelines For RituximabDocumento9 pagineGuidelines For RituximabMonica MonikaNessuna valutazione finora
- كيمياء سريرية 16Documento15 pagineكيمياء سريرية 16Aya AshrafNessuna valutazione finora
- Antimalarial Drug CologyDocumento15 pagineAntimalarial Drug CologyManthan ChauhanNessuna valutazione finora
- Peptic Ulcer ManagementDocumento51 paginePeptic Ulcer ManagementVincent SerNessuna valutazione finora
- Bioassay of AcetylcholineDocumento1 paginaBioassay of AcetylcholineSangi RajNessuna valutazione finora
- Cytotoxic ChemotherapyDocumento33 pagineCytotoxic ChemotherapyDoniTrinandaNessuna valutazione finora
- Pharmacotherapeutics - PharmD II YearDocumento5 paginePharmacotherapeutics - PharmD II YearSuresh Thanneru100% (2)
- AzathioprineDocumento3 pagineAzathioprineAdela abboudNessuna valutazione finora
- Corticosteroids and Antagonists 25-08-22Documento35 pagineCorticosteroids and Antagonists 25-08-22Uzma KhanNessuna valutazione finora
- CorticosteroidsDocumento40 pagineCorticosteroidsBusy worldNessuna valutazione finora
- 29th Convocation Souvenir 2020 (Batch 2016-17)Documento75 pagine29th Convocation Souvenir 2020 (Batch 2016-17)Tabish KhalidNessuna valutazione finora
- HCIA SECURITY Searchable PDFDocumento294 pagineHCIA SECURITY Searchable PDFgurungeNessuna valutazione finora
- $daily UCE Protect IP Block ListDocumento295 pagine$daily UCE Protect IP Block ListTabish KhalidNessuna valutazione finora
- Advisory Committee Onartificail IntelligenceDocumento1 paginaAdvisory Committee Onartificail IntelligenceTabish KhalidNessuna valutazione finora
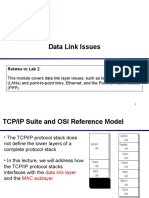
- Data Link Issues: Relates To Lab 2Documento17 pagineData Link Issues: Relates To Lab 2Tabish KhalidNessuna valutazione finora
- Final AOS SPR 2018Documento2 pagineFinal AOS SPR 2018Tabish KhalidNessuna valutazione finora
- Stages in Somatostatin Synthesis:: Reading FrameDocumento2 pagineStages in Somatostatin Synthesis:: Reading FrameTabish KhalidNessuna valutazione finora
- App Phy PH-121 2011Documento2 pagineApp Phy PH-121 2011Tabish KhalidNessuna valutazione finora
- Arch BarDocumento28 pagineArch BarFachrul Latif DentistNessuna valutazione finora
- 4 Steps: Instrument PassingDocumento3 pagine4 Steps: Instrument PassingGwyn Leen CagasNessuna valutazione finora
- Total Hip ReplacementDocumento152 pagineTotal Hip Replacementminas100% (3)
- Clinical Case Presentation:: Premature Rupture of MembranesDocumento31 pagineClinical Case Presentation:: Premature Rupture of Membranesjoshua remonNessuna valutazione finora
- Wen Bing2Documento9 pagineWen Bing2Jaffer Aftab0% (1)
- How Is Turner Syndrome DiagnosedDocumento9 pagineHow Is Turner Syndrome DiagnosedAnonymous lKO78aNessuna valutazione finora
- American College of Women's Health PhysiciansDocumento16 pagineAmerican College of Women's Health PhysiciansSex & Gender Women's Health CollaborativeNessuna valutazione finora
- Clomifen Citrat PDFDocumento9 pagineClomifen Citrat PDFGilang Andhika SNessuna valutazione finora
- Metaplasia of Fgtract & Recent AdvancesDocumento62 pagineMetaplasia of Fgtract & Recent AdvancesGaurav Pawar100% (4)
- Anatomy & Physiology Eye: By: DR Abdul Salim Ismail Ophthalmology Department Hospital Pulau Pinang 8 July 2015Documento35 pagineAnatomy & Physiology Eye: By: DR Abdul Salim Ismail Ophthalmology Department Hospital Pulau Pinang 8 July 2015muhammadridhwanNessuna valutazione finora
- Stomach Ulceration Leaflet and Drugs Used To Treat Peptic Ulcer DiseaseDocumento4 pagineStomach Ulceration Leaflet and Drugs Used To Treat Peptic Ulcer DiseasePrisma TridaNessuna valutazione finora
- Clinical Laboratory Critical Value List: Page 1 of 2Documento2 pagineClinical Laboratory Critical Value List: Page 1 of 2소여리Nessuna valutazione finora
- CholecystitisDocumento12 pagineCholecystitisMariela HuertaNessuna valutazione finora
- Smart Phone For Shade Selection in Fixed ProsthodonticsDocumento2 pagineSmart Phone For Shade Selection in Fixed ProsthodonticsRajsandeep SinghNessuna valutazione finora
- Asphyxia NeonatorumDocumento35 pagineAsphyxia NeonatorumMuhammad RagilNessuna valutazione finora
- Reconstruction of Posttraumatic Disorders of The ForearmDocumento12 pagineReconstruction of Posttraumatic Disorders of The Forearmsinung bawonoNessuna valutazione finora
- 4f4f3d97-3c1c-49d9-8f67-7c1bd1d9f142Documento325 pagine4f4f3d97-3c1c-49d9-8f67-7c1bd1d9f142James CapplemanNessuna valutazione finora
- TTNDocumento10 pagineTTNsiti nur indahNessuna valutazione finora
- PheochromocytomaDocumento6 paginePheochromocytomaSonya YuNessuna valutazione finora
- Eye Exams For ChildrenDocumento5 pagineEye Exams For ChildrenDanielz FranceNessuna valutazione finora
- Undescended Testicles, Retractile Testicles, and Testicular TorsionDocumento7 pagineUndescended Testicles, Retractile Testicles, and Testicular TorsionYudhistira SuryamanggalaNessuna valutazione finora
- 10 Fascinating Facts About SurgeryDocumento11 pagine10 Fascinating Facts About SurgeryArlynn Lontoc De RamosNessuna valutazione finora
- Vulvar Care e PDFDocumento9 pagineVulvar Care e PDFainurrohmaniyahNessuna valutazione finora
- Anhydramnios - Radiology Reference Article - RadiopaediaDocumento9 pagineAnhydramnios - Radiology Reference Article - RadiopaediaMuhammad IqsanNessuna valutazione finora
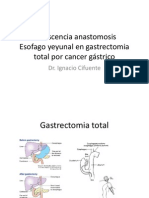
- Dehiscencia Anastomosis Esofago Yeyunal en Gastrectomia Total Por Cancer GástricoDocumento22 pagineDehiscencia Anastomosis Esofago Yeyunal en Gastrectomia Total Por Cancer GástriconachooooooooNessuna valutazione finora
- Minor Cases of Piolo PascualDocumento3 pagineMinor Cases of Piolo PascualdonzkieNessuna valutazione finora
- H. Hypertensive Disorders in PregnancyDocumento50 pagineH. Hypertensive Disorders in PregnancyRadha ChiombonNessuna valutazione finora
- Trigonum Colli AnteriusDocumento13 pagineTrigonum Colli Anteriusyati rosmiatiNessuna valutazione finora
- Anexa 1A IMM UltraDocumento15 pagineAnexa 1A IMM UltraGabriela Diana MedlineNessuna valutazione finora
- A1 All ProgramsDocumento28 pagineA1 All ProgramsRaniel John Avila SampianoNessuna valutazione finora