Potrebbero piacerti anche
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- RUBEEEEDocumento44 pagineRUBEEEEAhlyssa de JorgeNessuna valutazione finora
- Brenda Alderman v. The Philadelphia Housing Authority, 496 F.2d 164, 3rd Cir. (1974)Documento16 pagineBrenda Alderman v. The Philadelphia Housing Authority, 496 F.2d 164, 3rd Cir. (1974)Scribd Government DocsNessuna valutazione finora
- The Presidential ScandalsDocumento328 pagineThe Presidential ScandalsDr Nasser AfifyNessuna valutazione finora
- LTRC FInal Report 558 Development of Performance-Based Specifications For Louisiana Asphalt MixturesDocumento149 pagineLTRC FInal Report 558 Development of Performance-Based Specifications For Louisiana Asphalt MixtureswalaywanNessuna valutazione finora
- Bottoms y Sparks - Legitimacy - and - Imprisonment - Revisited PDFDocumento29 pagineBottoms y Sparks - Legitimacy - and - Imprisonment - Revisited PDFrossana gaunaNessuna valutazione finora
- Att.3 Training Evaluation For Course Trainer & FacilitiesDocumento2 pagineAtt.3 Training Evaluation For Course Trainer & FacilitiesYusufNessuna valutazione finora
- ComeniusDocumento38 pagineComeniusDora ElenaNessuna valutazione finora
- Teacher LOA & TermsDocumento3 pagineTeacher LOA & TermsMike SchmoronoffNessuna valutazione finora
- SMF Update Barang 05 Desember 2022Documento58 pagineSMF Update Barang 05 Desember 2022Apotek Ibnu RusydNessuna valutazione finora
- Psychology ProjectDocumento7 paginePsychology Projectsai indiraNessuna valutazione finora
- HistogramDocumento7 pagineHistogramTesfaye MinaleNessuna valutazione finora
- MULTIPLE CHOICE. Choose The One Alternative That Best Completes The Statement or Answers The QuestionDocumento6 pagineMULTIPLE CHOICE. Choose The One Alternative That Best Completes The Statement or Answers The QuestionBoshra BoshraNessuna valutazione finora
- 1st Annual Charity Golf Tournament For ChloeDocumento2 pagine1st Annual Charity Golf Tournament For ChloeM.G. PerezNessuna valutazione finora
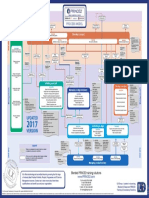
- p2 Process Model 2017Documento1 paginap2 Process Model 2017Miguel Fernandes0% (1)
- TENSES ExerciseDocumento28 pagineTENSES ExerciseKhanh PhamNessuna valutazione finora
- Project RealDocumento4 pagineProject RealKenneth Jay BagandoNessuna valutazione finora
- HRM848 Training Techniques and Practices Summer 2021Documento39 pagineHRM848 Training Techniques and Practices Summer 2021Dhruvi RajNessuna valutazione finora
- Global SAP Access and Operations Workplan v7-2017 ERPDocumento87 pagineGlobal SAP Access and Operations Workplan v7-2017 ERPJenniferNessuna valutazione finora
- Cinderella: From The Blue Fairy Book of Andrew LangDocumento7 pagineCinderella: From The Blue Fairy Book of Andrew LangnizamianNessuna valutazione finora
- Slides - Simple Linear RegressionDocumento35 pagineSlides - Simple Linear RegressionJarir AhmedNessuna valutazione finora
- Final Exam1-Afternoon SessionDocumento40 pagineFinal Exam1-Afternoon SessionJoshua Wright0% (1)
- Chapter02 AnglesDocumento40 pagineChapter02 Angleslen16328100% (1)
- Skills For Developing Yourself As A LeaderDocumento26 pagineSkills For Developing Yourself As A LeaderhIgh QuaLIty SVTNessuna valutazione finora
- Level - 1: Expansion of DeterminantsDocumento13 pagineLevel - 1: Expansion of DeterminantsAtomitronNessuna valutazione finora
- HaDocumento15 pagineHaNicole Easther GabilangosoNessuna valutazione finora
- Thompson VarelaDocumento18 pagineThompson VarelaGiannis NinosNessuna valutazione finora
- Approaching Checklist Final PDFDocumento15 pagineApproaching Checklist Final PDFCohort Partnerships100% (1)
- SSPC - Guia 12Documento6 pagineSSPC - Guia 12José Alvaro Herrera Ramos50% (2)
- SCHEEL, Bernd - Egyptian Metalworking and ToolsDocumento36 pagineSCHEEL, Bernd - Egyptian Metalworking and ToolsSamara Dyva86% (7)
- Lab Exercise: 8Documento5 pagineLab Exercise: 8Test UserNessuna valutazione finora