Potrebbero piacerti anche
- Understanding Chronic Kidney Disease: A guide for the non-specialistDa EverandUnderstanding Chronic Kidney Disease: A guide for the non-specialistValutazione: 4 su 5 stelle4/5 (3)
- Kidney Disease Acute and Chronic 2019Documento60 pagineKidney Disease Acute and Chronic 2019salamon2tNessuna valutazione finora
- Complementary and Alternative Medical Lab Testing Part 8: UrologyDa EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyValutazione: 3 su 5 stelle3/5 (1)
- National Leaflet About CKD and eGFR For GPs (Updated September 2007)Documento2 pagineNational Leaflet About CKD and eGFR For GPs (Updated September 2007)Dhika ArdiansyahNessuna valutazione finora
- Chronic Kidney Disease (CKD) : Provider's Guide To Diagnose and Code CKDDocumento2 pagineChronic Kidney Disease (CKD) : Provider's Guide To Diagnose and Code CKDAry Rio PambudiNessuna valutazione finora
- CKD SheetDocumento4 pagineCKD SheetMomy SutanNessuna valutazione finora
- Akt RenalDocumento4 pagineAkt Renaldzidek7Nessuna valutazione finora
- Kidney JWQJDHGWDJQWHGJWQDGJWGDocumento2 pagineKidney JWQJDHGWDJQWHGJWQDGJWGJess L PayagNessuna valutazione finora
- CKD Kdigo 2012Documento27 pagineCKD Kdigo 2012giggs_libraNessuna valutazione finora
- Cumbria and Lancs KCN Algorithm PDFDocumento18 pagineCumbria and Lancs KCN Algorithm PDFratih83Nessuna valutazione finora
- CKD PDFDocumento20 pagineCKD PDFReyhan TarisNessuna valutazione finora
- PCP in A Box - Module 1Documento43 paginePCP in A Box - Module 1Fate ChanNessuna valutazione finora
- Chronic Kidney DiseaseDocumento39 pagineChronic Kidney DiseaseAgatha RogerNessuna valutazione finora
- Chronic Kidney DiseaseDocumento24 pagineChronic Kidney DiseasepradeepnagdaNessuna valutazione finora
- Chronic Kidney Disease ReferalDocumento3 pagineChronic Kidney Disease ReferalsumiranprabhuNessuna valutazione finora
- Chronic Kidney Disease: Rizki Aliana AgustinaDocumento85 pagineChronic Kidney Disease: Rizki Aliana AgustinaRofi IrmanNessuna valutazione finora
- CKD CHCRTDocumento28 pagineCKD CHCRTNurhidayati KeriyunNessuna valutazione finora
- Chronic Kidney DiseaseDocumento14 pagineChronic Kidney DiseaseJoel CanenciaNessuna valutazione finora
- PPT CKDDocumento35 paginePPT CKDCandice LavigneNessuna valutazione finora
- Diabetic NephropathyDocumento38 pagineDiabetic NephropathyMade Widiastika100% (1)
- Indications For Initiation of DialysisDocumento11 pagineIndications For Initiation of DialysisMilton BenevidesNessuna valutazione finora
- Diagnosis Aki Dan CKDDocumento39 pagineDiagnosis Aki Dan CKDEly Kartika100% (1)
- CKD 2016Documento39 pagineCKD 2016husnaNessuna valutazione finora
- Chronic Kidney DiseaseDocumento42 pagineChronic Kidney DiseaseLeta GemechuNessuna valutazione finora
- 02-50-4079 ABB ManagingTransRecipBk PC PDFDocumento12 pagine02-50-4079 ABB ManagingTransRecipBk PC PDFjulma1306Nessuna valutazione finora
- Chronic Kidney Disease ReferalDocumento3 pagineChronic Kidney Disease ReferalAnonymous MpBxSgpwNessuna valutazione finora
- Chronic Kidney Disease ReferalDocumento3 pagineChronic Kidney Disease ReferalAnonymous MpBxSgpwNessuna valutazione finora
- CKD MedscapeDocumento65 pagineCKD MedscapeLuses Shantia HaryantoNessuna valutazione finora
- Chronic Kidney DiseaseDocumento39 pagineChronic Kidney DiseaseGumarbio Setiadi Zakaria100% (1)
- How To Improve Outcomes in Hemodialysis PatientsDocumento24 pagineHow To Improve Outcomes in Hemodialysis PatientsSuardy CiayadiNessuna valutazione finora
- National Leaflet About CKD and eGFR For GPs Updated September 2007 PDFDocumento2 pagineNational Leaflet About CKD and eGFR For GPs Updated September 2007 PDFRifky Octavio PNessuna valutazione finora
- Diagnosa Penyakit Ginjal Kronik Dan Indikasi TPG RRTDocumento56 pagineDiagnosa Penyakit Ginjal Kronik Dan Indikasi TPG RRTASIS ADRINessuna valutazione finora
- Patofisiologi Penyakit Ginjal KronikDocumento35 paginePatofisiologi Penyakit Ginjal KronikEgy Sunanda Putra Direktorat Poltekkes JambiNessuna valutazione finora
- Chronic Kidney Disease: The BasicsDocumento56 pagineChronic Kidney Disease: The BasicsAlmas Safina KauserNessuna valutazione finora
- Curs 5 Nefro Boala Cronica de RinichiDocumento113 pagineCurs 5 Nefro Boala Cronica de RinichiAdriana Vladutu100% (2)
- The Primary/secondary Care InterfaceDocumento48 pagineThe Primary/secondary Care InterfaceHadiri Imam MNessuna valutazione finora
- Chronic Kidney Disease Bhakti MuliaDocumento24 pagineChronic Kidney Disease Bhakti MuliaCOVID RSHJNessuna valutazione finora
- Chronickidneydiseaseinthe Elderly: Thin Thin Maw,, Linda FriedDocumento14 pagineChronickidneydiseaseinthe Elderly: Thin Thin Maw,, Linda Friedkhangha.ptNessuna valutazione finora
- Chronic Kidney Disease - EMEDICINE 3020.docx.2021Documento56 pagineChronic Kidney Disease - EMEDICINE 3020.docx.2021qayyum consultantfpscNessuna valutazione finora
- Preventif CKD FinalDocumento43 paginePreventif CKD Finaltika.dyahmustikaNessuna valutazione finora
- Kdigo 2013. CKDDocumento110 pagineKdigo 2013. CKDcvsmed100% (1)
- CKD Pocket GuideDocumento2 pagineCKD Pocket GuideLutfi MalefoNessuna valutazione finora
- Chronic Kidney DiseaseDocumento14 pagineChronic Kidney DiseaseFernando SugiartoNessuna valutazione finora
- DefisniDocumento41 pagineDefisniAzizah MNessuna valutazione finora
- CKD CmeDocumento45 pagineCKD Cmeizatul farhanahNessuna valutazione finora
- 12B. Kuliah CKD 2017Documento44 pagine12B. Kuliah CKD 2017yussikafernandaNessuna valutazione finora
- Class 2: ECE-Rft Part 2, VitaminsDocumento85 pagineClass 2: ECE-Rft Part 2, VitaminsammuNessuna valutazione finora
- Chronic Kidney Disease: Presented By, Mariya Antony 3 Year BSC Nursing ST - Thomas College of Nursing ChethipuzhaDocumento62 pagineChronic Kidney Disease: Presented By, Mariya Antony 3 Year BSC Nursing ST - Thomas College of Nursing ChethipuzhaSamuel LalNessuna valutazione finora
- Stop-Acei Trial Journal ClubDocumento3 pagineStop-Acei Trial Journal Clubapi-648891519Nessuna valutazione finora
- CS - Step 2 - Feline Kidney DiseaseDocumento2 pagineCS - Step 2 - Feline Kidney DiseaseShar ThornNessuna valutazione finora
- Identification of CKD: Algorithm ADocumento3 pagineIdentification of CKD: Algorithm ArawanNessuna valutazione finora
- Part 9. Approach To Chronic Kidney Disease Using These GuidelinesDocumento8 paginePart 9. Approach To Chronic Kidney Disease Using These GuidelinesSudjarwo AntonNessuna valutazione finora
- Diabetes English - 200416 PDFDocumento24 pagineDiabetes English - 200416 PDFIulia NegruNessuna valutazione finora
- CKD UnsoedDocumento42 pagineCKD UnsoedSutan Malik IbrahimNessuna valutazione finora
- Delaying or Halting Progression of Chronic Kidney DiseaseDocumento9 pagineDelaying or Halting Progression of Chronic Kidney Diseasehannya manNessuna valutazione finora
- ACCP 2018 NephrologyDocumento31 pagineACCP 2018 NephrologyMonica Febri Andari100% (1)
- Mayoclinproc 84 2 012 PDFDocumento7 pagineMayoclinproc 84 2 012 PDFVinceErwinTanNessuna valutazione finora
- Chronic Kidney Disease (CKD) in Children: DR Saiel Al Sarhan MD, PHDDocumento48 pagineChronic Kidney Disease (CKD) in Children: DR Saiel Al Sarhan MD, PHDMAYSAA HamarnehNessuna valutazione finora
- Feline Chronic Kidney Disease - Integrated ApproachDocumento12 pagineFeline Chronic Kidney Disease - Integrated ApproachClara SanchezNessuna valutazione finora
- Chronic Kidney Disease in Small Animals1Documento16 pagineChronic Kidney Disease in Small Animals1ZiedTrikiNessuna valutazione finora
- Dell Inspirion 15 5551 Compal LA-B912P r1.0Documento42 pagineDell Inspirion 15 5551 Compal LA-B912P r1.0Warren DonaldsonNessuna valutazione finora
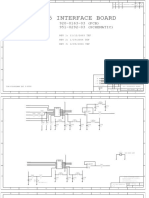
- 920-0163-03, 951-0292-03, Q45 INTERFACE (Q45 INTERFACE BOARD) Rev 3, 04.09.2004Documento26 pagine920-0163-03, 951-0292-03, Q45 INTERFACE (Q45 INTERFACE BOARD) Rev 3, 04.09.2004Warren DonaldsonNessuna valutazione finora
- Dell Inspiron 17 5755 Compal LA-C142P r1.0 AMDDocumento56 pagineDell Inspiron 17 5755 Compal LA-C142P r1.0 AMDWarren Donaldson100% (1)
- Shock Handout NurseDocumento9 pagineShock Handout NurseWarren DonaldsonNessuna valutazione finora
- Networking A Beginner's GuideDocumento36 pagineNetworking A Beginner's Guidez4rm4rNessuna valutazione finora
- Next7P12-GP Tech Spec 102412Documento4 pagineNext7P12-GP Tech Spec 102412Warren DonaldsonNessuna valutazione finora
- Samsung Gt-p3100 r0.6 SchematicsDocumento11 pagineSamsung Gt-p3100 r0.6 SchematicsWarren Donaldson100% (1)
- Business PlanDocumento21 pagineBusiness PlanWarren DonaldsonNessuna valutazione finora
- Fukuoka Kinen HospitalDocumento23 pagineFukuoka Kinen HospitaldihcsarNessuna valutazione finora
- Carriere Motion Appliance Brochure InternationalDocumento8 pagineCarriere Motion Appliance Brochure InternationalOrtho OrganizersNessuna valutazione finora
- CG A013 04 Stainless Steel Crowns in Deciduous MolarsDocumento5 pagineCG A013 04 Stainless Steel Crowns in Deciduous MolarsmahmoudNessuna valutazione finora
- Medical and Health Care DocumentDocumento6 pagineMedical and Health Care Document786waqar786Nessuna valutazione finora
- Conivaptan MedicalDocumento38 pagineConivaptan MedicalSanjay NavaleNessuna valutazione finora
- KONDROSARKOMADocumento18 pagineKONDROSARKOMAMangGun-gunGunawanNessuna valutazione finora
- Medical DoctorsDocumento4 pagineMedical DoctorsMiko MiguelNessuna valutazione finora
- (Essentials in Ophthalmology) Ahmad A. Aref, Rohit Varma (Eds.) - Advanced Glaucoma Surgery-Springer International Publishing (2015)Documento140 pagine(Essentials in Ophthalmology) Ahmad A. Aref, Rohit Varma (Eds.) - Advanced Glaucoma Surgery-Springer International Publishing (2015)Inna Bujor100% (1)
- Pit and Fissure Sealant in Prevention of Dental CariesDocumento4 paginePit and Fissure Sealant in Prevention of Dental CariesSyuhadaSetiawanNessuna valutazione finora
- 1 Original ArticleDocumento4 pagine1 Original ArticlejessicaNessuna valutazione finora
- The 6-Elements Orthodontic PhilosophyDocumento5 pagineThe 6-Elements Orthodontic PhilosophymutansNessuna valutazione finora
- Ptrs 06 113Documento7 paginePtrs 06 113ahmetrixNessuna valutazione finora
- Behavioral Treatment For Nocturnal EnuresisDocumento8 pagineBehavioral Treatment For Nocturnal EnuresispopoviciaidaNessuna valutazione finora
- Facial ContoursDocumento20 pagineFacial Contourscmkflorida7011100% (1)
- (PPT) Oral Health and Down SyndromeDocumento31 pagine(PPT) Oral Health and Down SyndromeMuabhiNessuna valutazione finora
- Esthetics in Removable Partial Denture - A ReviewDocumento5 pagineEsthetics in Removable Partial Denture - A Reviewnissadhania100% (1)
- AhmedabadDocumento39 pagineAhmedabadacme financialNessuna valutazione finora
- Physiotherapy in Pediatrics - NEURO MUSCULAR CONDITIONSDocumento28 paginePhysiotherapy in Pediatrics - NEURO MUSCULAR CONDITIONSKumar G PalaniNessuna valutazione finora
- El-Chaar - Introduction To Pediatric PharmacotherapyDocumento85 pagineEl-Chaar - Introduction To Pediatric PharmacotherapyTaj PolinNessuna valutazione finora
- Guideline Clinical RotationsDocumento39 pagineGuideline Clinical RotationsMaria ulfahNessuna valutazione finora
- The Maryland Bridge OrginalDocumento34 pagineThe Maryland Bridge OrginalMohammed AmeenNessuna valutazione finora
- Treatment Planning of The Edentulous Mandible PDFDocumento9 pagineTreatment Planning of The Edentulous Mandible PDFHugoMoralesTecnicoDentalNessuna valutazione finora
- Qi 29 6 Dubojska 7Documento6 pagineQi 29 6 Dubojska 7DrSumit MisraNessuna valutazione finora
- Anatomy of The Lingual Vestibule and Its Influence On Denture Borders 2161 0940.1000122Documento4 pagineAnatomy of The Lingual Vestibule and Its Influence On Denture Borders 2161 0940.1000122Purnama SyahbaniNessuna valutazione finora
- Atlas of Cataract SurgeryDocumento196 pagineAtlas of Cataract SurgeryDaniel Fernández Gajardo100% (3)
- Journal of Clinical and Medical ImagesDocumento3 pagineJournal of Clinical and Medical Imagesliterature publishersNessuna valutazione finora
- Sharpening The Equity Focus: Selected Innovations and Lessons Learned From UNICEF-assisted Programmes 2009-2010Documento80 pagineSharpening The Equity Focus: Selected Innovations and Lessons Learned From UNICEF-assisted Programmes 2009-2010UNICEFNessuna valutazione finora
- Frequently Asked Questions On The Referral To Treatment (RTT) Data CollectionDocumento24 pagineFrequently Asked Questions On The Referral To Treatment (RTT) Data Collectionraduben5403Nessuna valutazione finora
- Health Care To Rural Population in Russian FederationDocumento8 pagineHealth Care To Rural Population in Russian FederationbrightagbotuiNessuna valutazione finora
- Stage 1: Dorsal Induction: Pediatric NeuroradiologyDocumento8 pagineStage 1: Dorsal Induction: Pediatric Neuroradiologysarguss14100% (1)