Potrebbero piacerti anche
- n378.008 Iris Website Staging of CKD PDFDocumento8 paginen378.008 Iris Website Staging of CKD PDFrutebeufNessuna valutazione finora
- Dr. Sunatrio - Management Hypovolemic ShockDocumento59 pagineDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeNessuna valutazione finora
- CiprofloxacinDocumento2 pagineCiprofloxacinNika Joy Cabrera AlarconNessuna valutazione finora
- Kolestasis Intrahepatal Vs EkstrahepatalDocumento4 pagineKolestasis Intrahepatal Vs EkstrahepatalrikarikaNessuna valutazione finora
- Gangguan Involuntary MovementDocumento54 pagineGangguan Involuntary MovementMuammar RizkiNessuna valutazione finora
- Zoledronic AcidDocumento7 pagineZoledronic AcidbabiNessuna valutazione finora
- Cor PulmonaleDocumento42 pagineCor PulmonaleNym Angga SantosaNessuna valutazione finora
- Hopkins Medicine Review Cardiology SectionDocumento54 pagineHopkins Medicine Review Cardiology SectiondrsalilsidhqueNessuna valutazione finora
- Management of HypokalemiaDocumento6 pagineManagement of HypokalemiaEsraa Abu elelaNessuna valutazione finora
- Hypovolemic Shock and DicDocumento53 pagineHypovolemic Shock and Dicapi-3743483100% (6)
- Notes On History Taking in The Cardiovascular SystemDocumento10 pagineNotes On History Taking in The Cardiovascular Systemmdjohar72Nessuna valutazione finora
- XI. Chronic Kidney Disease PDFDocumento45 pagineXI. Chronic Kidney Disease PDFnaro ayosNessuna valutazione finora
- G 6 PDDocumento45 pagineG 6 PDPat TuazonNessuna valutazione finora
- Kriteria Diagnosis RBBB - LBBBDocumento1 paginaKriteria Diagnosis RBBB - LBBBDwitya RiliantiNessuna valutazione finora
- Kegawatan Respirasi May2016-FkumyDocumento62 pagineKegawatan Respirasi May2016-FkumyAgustina Tri P. DNessuna valutazione finora
- Pericardial EffusionDocumento36 paginePericardial EffusionRizky Amalia Wakano100% (1)
- Dengue Hemorrhagic Fever (DHF)Documento9 pagineDengue Hemorrhagic Fever (DHF)Muhamad Hilal Rizki KusumaNessuna valutazione finora
- Djenkolism ToxificationDocumento5 pagineDjenkolism ToxificationSilvia RizkaNessuna valutazione finora
- WHO Dengue Classification and Case Management-FlyerDocumento2 pagineWHO Dengue Classification and Case Management-FlyerKathleen DyNessuna valutazione finora
- Anti Angina (Hany)Documento51 pagineAnti Angina (Hany)Angga AhadiyatNessuna valutazione finora
- CYSTOSTOMYDocumento60 pagineCYSTOSTOMYOepil KirickNessuna valutazione finora
- Venous Thromboembolism (VTE) - McMaster Pathophysiology ReviewDocumento9 pagineVenous Thromboembolism (VTE) - McMaster Pathophysiology ReviewFadiyah UlfahNessuna valutazione finora
- EKG PJK Co AssDocumento115 pagineEKG PJK Co AsssalmaNessuna valutazione finora
- Extubation Criteria & Delayed EmergenceDocumento3 pagineExtubation Criteria & Delayed EmergenceAnonymous OlS0WZwNessuna valutazione finora
- Warfarin Mechanism of ActionDocumento7 pagineWarfarin Mechanism of ActionIna GrigorasNessuna valutazione finora
- A Case Study of Epidural HematomaDocumento27 pagineA Case Study of Epidural HematomaNeil GoNessuna valutazione finora
- Congestive Heart Failure PDFDocumento49 pagineCongestive Heart Failure PDFVerinice NañascaNessuna valutazione finora
- The Renin Angiotensin Aldosterone System (RAAS)Documento22 pagineThe Renin Angiotensin Aldosterone System (RAAS)Chandra pranataNessuna valutazione finora
- InsulinomaDocumento16 pagineInsulinomaDerly Barino HasdiNessuna valutazione finora
- Alteplase PharmacologyDocumento24 pagineAlteplase Pharmacologysatyagraha84Nessuna valutazione finora
- Antibiotic Therapy For Peritonitis: Treatment Overview, Spontaneous Bacterial Peritonitis, Secondary and Tertiary PeritonitisDocumento7 pagineAntibiotic Therapy For Peritonitis: Treatment Overview, Spontaneous Bacterial Peritonitis, Secondary and Tertiary PeritonitisTias SubagioNessuna valutazione finora
- Encephalopaty UremicDocumento6 pagineEncephalopaty UremicMasriyaniNessuna valutazione finora
- Cakul - Emergency JantungDocumento8 pagineCakul - Emergency JantungRosalia Septaviana RisdiartaNessuna valutazione finora
- Drug EruptionDocumento46 pagineDrug EruptionSyahDikaNessuna valutazione finora
- HEMATOCHEZIADocumento26 pagineHEMATOCHEZIAAlvin HartantoNessuna valutazione finora
- Acs TrombolitikDocumento55 pagineAcs TrombolitikDiana IswardhaniNessuna valutazione finora
- 19 Anesthesia For Biliary AtresiaDocumento19 pagine19 Anesthesia For Biliary AtresiaDwiki Surya PrayogaNessuna valutazione finora
- Sick Sinus Syndrome 1Documento23 pagineSick Sinus Syndrome 1Salman HabeebNessuna valutazione finora
- HypokalemiaDocumento7 pagineHypokalemiaNader SmadiNessuna valutazione finora
- Alport SyndromeDocumento7 pagineAlport SyndromeNTA UGC-NET100% (1)
- MANAGEMENT ACUTE ISCHEMIC STROKE (Simpo rTPA RSHS) - LisdaDocumento63 pagineMANAGEMENT ACUTE ISCHEMIC STROKE (Simpo rTPA RSHS) - LisdadianNessuna valutazione finora
- Leukemia (Kuliah 2 Ipd III)Documento15 pagineLeukemia (Kuliah 2 Ipd III)Yon-SyuhandaNessuna valutazione finora
- Tehnik - Tehnik Analgesia Post OperasiDocumento32 pagineTehnik - Tehnik Analgesia Post OperasiGuntur Aryo PuntodewoNessuna valutazione finora
- NSTEMI Refarat Cardio 2016Documento48 pagineNSTEMI Refarat Cardio 2016Anonymous IOkNvM8VbtNessuna valutazione finora
- Pathophysiology of Breast CancerDocumento8 paginePathophysiology of Breast CancerNicole Villanueva, BSN - Level 3ANessuna valutazione finora
- Infective Endocarditis: Ainal Fadly Adigama PF Enny SuryantiDocumento50 pagineInfective Endocarditis: Ainal Fadly Adigama PF Enny SuryantiFaisal Reza AdiebNessuna valutazione finora
- Referat Malaria SerebralDocumento42 pagineReferat Malaria SerebralLivia HanisamurtiNessuna valutazione finora
- Norepinephrine Drug StudyDocumento2 pagineNorepinephrine Drug StudyIrish LigayaNessuna valutazione finora
- Pneumonperitoneum A Review of Nonsurgical Causes PDFDocumento7 paginePneumonperitoneum A Review of Nonsurgical Causes PDFDellysa Eka Nugraha TNessuna valutazione finora
- Case Presentation: Alcoholic GastritisDocumento18 pagineCase Presentation: Alcoholic Gastritisstancy thomas100% (1)
- Thyroid StormDocumento16 pagineThyroid StormRaquid MariaNessuna valutazione finora
- Glucose Tolerance TestDocumento3 pagineGlucose Tolerance TestdechychyNessuna valutazione finora
- Intestinal ObstructionDocumento12 pagineIntestinal ObstructionNurul Nurnita100% (1)
- Acute Cholecystitis Ppt. DR Dilip S. RajpalDocumento42 pagineAcute Cholecystitis Ppt. DR Dilip S. Rajpaldiliprajpal73100% (1)
- HepatomegalyDocumento2 pagineHepatomegalyFuyumi RiaNessuna valutazione finora
- Atrial Septal Defect (ASD)Documento22 pagineAtrial Septal Defect (ASD)Akbar Iskandar100% (1)
- K - 7 Atrial Flutter (IKA)Documento8 pagineK - 7 Atrial Flutter (IKA)thomasfelixNessuna valutazione finora
- K7 - Supraventricular Tachycardia (SVT)Documento44 pagineK7 - Supraventricular Tachycardia (SVT)Zikri Putra Lan LubisNessuna valutazione finora
- Cardiac ArrythmiaDocumento16 pagineCardiac ArrythmiaHossen AliNessuna valutazione finora
- Anaesthesia and Atrial FibrillationDocumento15 pagineAnaesthesia and Atrial FibrillationNaresh Dhawan100% (1)
- Avnrt AvrtDocumento21 pagineAvnrt AvrtRima Rovanne Wenas100% (1)
- Heart Diseases in PregnancyDocumento19 pagineHeart Diseases in PregnancyKirubah Sai PatnaikNessuna valutazione finora
- PT Management & Problems of The CV System - Part 4 Cheat SheetDocumento2 paginePT Management & Problems of The CV System - Part 4 Cheat SheetKat KatNessuna valutazione finora
- Handouts - Cardio - Dr. Arreglo (Nov 2023)Documento92 pagineHandouts - Cardio - Dr. Arreglo (Nov 2023)Paola Jane OrioNessuna valutazione finora
- Ecg QuizDocumento46 pagineEcg QuizAchmad Jauhar FirdausNessuna valutazione finora
- Atrijalna Fibrilacija I FlaterDocumento3 pagineAtrijalna Fibrilacija I FlaterАлександар ПејчићNessuna valutazione finora
- Answers MediDocumento443 pagineAnswers MediAmine Younis100% (13)
- CVS Case SheetDocumento11 pagineCVS Case SheetSANA100% (1)
- IGNOU - School of Health Sciences (SOHS) - Programmes - Regular - Post-Graduate Diploma in Clinical Cardiology (PGDCC)Documento4 pagineIGNOU - School of Health Sciences (SOHS) - Programmes - Regular - Post-Graduate Diploma in Clinical Cardiology (PGDCC)Anonymous FCKe2lSgtNessuna valutazione finora
- JournalDocumento4 pagineJournalfinity de diosNessuna valutazione finora
- Hypertension GuidelinesDocumento1 paginaHypertension GuidelinesJuhne GioNessuna valutazione finora
- Mortality RateDocumento5 pagineMortality RateAlquino Heart RubioNessuna valutazione finora
- CHFDocumento35 pagineCHFNurayunie Abd HalimNessuna valutazione finora
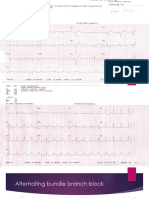
- Alternating Bundle Branch BlockDocumento9 pagineAlternating Bundle Branch BlockSyifa Mahmud Syukran AkbarNessuna valutazione finora
- Emergency Ultrasound EUS 教學Documento21 pagineEmergency Ultrasound EUS 教學juice119Nessuna valutazione finora
- WORKSHOP 30th ASMIHA - 13 Oktober 2021Documento22 pagineWORKSHOP 30th ASMIHA - 13 Oktober 2021Adhyt PratamaNessuna valutazione finora
- Myocardial Infarction With ST Segment ElevationDocumento27 pagineMyocardial Infarction With ST Segment ElevationRika Yulizah GobelNessuna valutazione finora
- Modes of Cardiac Pacing, Nomenclature and SelectionDocumento32 pagineModes of Cardiac Pacing, Nomenclature and SelectionMohammad AlmuhaiminNessuna valutazione finora
- OSCE Master List - CardiologyDocumento10 pagineOSCE Master List - CardiologyRebecca WongNessuna valutazione finora
- Diet For Cardiovaskular Disease - ErinetaDocumento8 pagineDiet For Cardiovaskular Disease - ErinetaErin NettaNessuna valutazione finora
- ECG MonitoringDocumento75 pagineECG MonitoringSanvar Mal SoniNessuna valutazione finora
- Block Kode CDC: Hypertensive Heart Disease With CHF (HHD)Documento5 pagineBlock Kode CDC: Hypertensive Heart Disease With CHF (HHD)Upi Ulfyah AprianiNessuna valutazione finora
- Try Out NewDocumento19 pagineTry Out NewIke AdrianaNessuna valutazione finora
- Aortic StenosisDocumento3 pagineAortic StenosisKhalid Mahmud Arifin100% (1)
- 118 Skills Lab-Week 2-ECG TakingDocumento8 pagine118 Skills Lab-Week 2-ECG TakingKeisha BartolataNessuna valutazione finora
- Concept Map Joshua ValdrizDocumento1 paginaConcept Map Joshua ValdrizJoshua ValdrizNessuna valutazione finora
- Chest Pain in Pediatrics: Tisha K. Yeh, MD and Jay Yeh, MDDocumento5 pagineChest Pain in Pediatrics: Tisha K. Yeh, MD and Jay Yeh, MDMahmoud AbouelsoudNessuna valutazione finora
- Exercise Tolerance TestDocumento15 pagineExercise Tolerance TestahmedNessuna valutazione finora
- Surgical Management of Coronary Artery DiseaseDocumento41 pagineSurgical Management of Coronary Artery Diseaseapi-19916399Nessuna valutazione finora
- Edward K. Chung M.D., F.A.C.P., F.A.C.C. (Auth.) - Ambulatory Electrocardiography - Holter Monitor Electrocardiography-Springer-Verlag New York (1979)Documento236 pagineEdward K. Chung M.D., F.A.C.P., F.A.C.C. (Auth.) - Ambulatory Electrocardiography - Holter Monitor Electrocardiography-Springer-Verlag New York (1979)Henrique MaiaNessuna valutazione finora