Potrebbero piacerti anche
- Maxillary Sinus Health DiseaseDocumento36 pagineMaxillary Sinus Health Diseasesaba mahrNessuna valutazione finora
- Faculty of Medicine Medical Education-Damietta University: Level 1 Semester IIDocumento34 pagineFaculty of Medicine Medical Education-Damietta University: Level 1 Semester IISounds of MindNessuna valutazione finora
- Nasal Discharge & ObstructionDocumento70 pagineNasal Discharge & ObstructionRajhmuniran KandasamyNessuna valutazione finora
- 3-Pharynx. Diseases of NasopharynxDocumento54 pagine3-Pharynx. Diseases of NasopharynxislamNessuna valutazione finora
- Differential DX of Nasal Obstruction & Neoplasms of Nose and PNSDocumento39 pagineDifferential DX of Nasal Obstruction & Neoplasms of Nose and PNSSubhada GosaviNessuna valutazione finora
- Diseases of Paranasal Sinuses-MayurDocumento36 pagineDiseases of Paranasal Sinuses-MayurMayur PawarNessuna valutazione finora
- Diseases of External Nose and Vestibulitis - 13th September 2021Documento33 pagineDiseases of External Nose and Vestibulitis - 13th September 2021Deepika LamichhaneNessuna valutazione finora
- 103 - Maxillary Sinus 1st YrDocumento38 pagine103 - Maxillary Sinus 1st Yrsanofazal786Nessuna valutazione finora
- Classifying and Treating Sinonasal TumorsDocumento25 pagineClassifying and Treating Sinonasal TumorsMariam QaisNessuna valutazione finora
- Kaki 13 Baru GantiDocumento7 pagineKaki 13 Baru Gantiandi akramNessuna valutazione finora
- Tumor Laring: Jenis, Anatomi, Faktor Resiko dan DiagnosisDocumento41 pagineTumor Laring: Jenis, Anatomi, Faktor Resiko dan DiagnosisM. NAUFAL RIZQI ALFANINessuna valutazione finora
- Benign and Malignant Tumors of Maxillary Sinus - AshishDocumento28 pagineBenign and Malignant Tumors of Maxillary Sinus - AshishKaran KhuranaNessuna valutazione finora
- Diseases of the External Nose: Classification, Diagnosis and TreatmentDocumento90 pagineDiseases of the External Nose: Classification, Diagnosis and TreatmentKamal Saud100% (2)
- Nasal Polyps Guide: Types, Causes, Symptoms & TreatmentDocumento26 pagineNasal Polyps Guide: Types, Causes, Symptoms & TreatmentAbdiqani MahdiNessuna valutazione finora
- Diseases of External Nose & Nasal VestibuleDocumento28 pagineDiseases of External Nose & Nasal VestibuleGAURAV100% (1)
- Diseases of External Nose and VestibuleDocumento45 pagineDiseases of External Nose and VestibuleNaseema273Nessuna valutazione finora
- Anatomy of Nasopharynx & AdenoidsDocumento3 pagineAnatomy of Nasopharynx & AdenoidsAmy KochNessuna valutazione finora
- SINONASAL Pres TariDocumento127 pagineSINONASAL Pres TariPradhana FwNessuna valutazione finora
- Nasopharyngeal AngiofibromaDocumento51 pagineNasopharyngeal Angiofibromakamal saudNessuna valutazione finora
- Diseases of AdenoidsDocumento19 pagineDiseases of AdenoidsMacktevin FraterinNessuna valutazione finora
- 18 Tonsil, Adenoid Notes Cumming Abd Key Topics (New Moe)Documento7 pagine18 Tonsil, Adenoid Notes Cumming Abd Key Topics (New Moe)osamaeNessuna valutazione finora
- Respiratory-Renal System Diseases GuideDocumento96 pagineRespiratory-Renal System Diseases Guidemina mounirNessuna valutazione finora
- Upper Respiratory Tract DiseasesDocumento34 pagineUpper Respiratory Tract DiseasesSounds of MindNessuna valutazione finora
- Nasal Tumors Classification and Key Benign GrowthsDocumento39 pagineNasal Tumors Classification and Key Benign Growthsmanoj kumarNessuna valutazione finora
- LMR Ent - Nose and Paransal SinusesDocumento7 pagineLMR Ent - Nose and Paransal SinusesYuku BabyNessuna valutazione finora
- Ent History Taking and Examination-1Documento16 pagineEnt History Taking and Examination-1Jyotirmayee100% (5)
- NoseDocumento37 pagineNoseDawit workalemNessuna valutazione finora
- Sinusitis 2 - New1Documento48 pagineSinusitis 2 - New1neferpitouhoeNessuna valutazione finora
- Nasopharyngeal Angiofibroma Treatment OptionsDocumento51 pagineNasopharyngeal Angiofibroma Treatment OptionsMiranda Yudhi CyubidubiduuNessuna valutazione finora
- 2 RHINOLOGY SinusDocumento87 pagine2 RHINOLOGY SinusWai Kwong ChiuNessuna valutazione finora
- NASAL SEPTUM DEVIATION: CAUSES, SYMPTOMS AND SURGICAL CORRECTIONDocumento105 pagineNASAL SEPTUM DEVIATION: CAUSES, SYMPTOMS AND SURGICAL CORRECTIONNguyễn ThànhNessuna valutazione finora
- Carcinoma MaxillaDocumento22 pagineCarcinoma MaxillaHAMSTRINGNessuna valutazione finora
- Madhukar NotesDocumento48 pagineMadhukar NotesMohan RajuNessuna valutazione finora
- Maxillary Sinus DR - AssefaDocumento65 pagineMaxillary Sinus DR - AssefaWorku KifleNessuna valutazione finora
- Tamil Nadu DR MGR Medical University ENT MBBS Prefinal Feb 2009 Question Paper With SolutionDocumento21 pagineTamil Nadu DR MGR Medical University ENT MBBS Prefinal Feb 2009 Question Paper With SolutionDr. T. BalasubramanianNessuna valutazione finora
- Maxillary Sinus Disease Diagnosis and TreatmentDocumento6 pagineMaxillary Sinus Disease Diagnosis and TreatmentevilllinNessuna valutazione finora
- Etiology and Classification of Periapical Tissue DiseasesDocumento5 pagineEtiology and Classification of Periapical Tissue DiseasesPrince AmiryNessuna valutazione finora
- اصلاحات کاربردی پزشکان عمومیDocumento23 pagineاصلاحات کاربردی پزشکان عمومیm1.nourianNessuna valutazione finora
- Histology: Diagnosis and Treatment of Chronic Apical AbscessDocumento3 pagineHistology: Diagnosis and Treatment of Chronic Apical AbscessPrince AmiryNessuna valutazione finora
- Shagubs EntDocumento25 pagineShagubs EntFelicianna Ashwinie StanleyNessuna valutazione finora
- Sino Nasal Polyposis SsDocumento42 pagineSino Nasal Polyposis SsJeffrinNessuna valutazione finora
- Anatomy of the Pharynx and LarynxDocumento33 pagineAnatomy of the Pharynx and LarynxFuad AwelNessuna valutazione finora
- Maxillary Sinus Anatomy and Oroantral FistulaDocumento26 pagineMaxillary Sinus Anatomy and Oroantral FistulaRobins DhakalNessuna valutazione finora
- ENT Urgencies / Emergencies in Primary CareDocumento55 pagineENT Urgencies / Emergencies in Primary CareDr_Aan_ArdiansyahNessuna valutazione finora
- ENT Notes CrakDocumento52 pagineENT Notes CrakGrant KimNessuna valutazione finora
- ENT Batch 2022 Annual Paper-1Documento9 pagineENT Batch 2022 Annual Paper-1mudassirahmedNessuna valutazione finora
- Head and Neck PPT 2024Documento65 pagineHead and Neck PPT 2024lallsNessuna valutazione finora
- Surgicaltreatmentofparaphyrngealandretropharyngealabscesses 170324144452Documento39 pagineSurgicaltreatmentofparaphyrngealandretropharyngealabscesses 170324144452MusabbirNessuna valutazione finora
- Adenoidectomy and Tonsillectomy 2Documento27 pagineAdenoidectomy and Tonsillectomy 2DR AAMNessuna valutazione finora
- Maxillary SinusDocumento108 pagineMaxillary SinusNitheesha MuthyalaNessuna valutazione finora
- 2a. Neck Swellings (U.G.)Documento83 pagine2a. Neck Swellings (U.G.)Raman Prasad SharmaNessuna valutazione finora
- Case Dr. Oscar - Sinusitis1Documento45 pagineCase Dr. Oscar - Sinusitis1haryo wiryantoNessuna valutazione finora
- Oral PathologyDocumento182 pagineOral PathologyPurnimaNessuna valutazione finora
- Anatomy and Disorders of the Nasal SeptumDocumento24 pagineAnatomy and Disorders of the Nasal SeptumAyush Paudel100% (1)
- Ear, Nose and Throat ConditionsDocumento10 pagineEar, Nose and Throat ConditionsSaileekitha AjamoniNessuna valutazione finora
- Nasopharyngeal AngiofibromaDocumento15 pagineNasopharyngeal AngiofibromaSiddiqur Rahman AkashNessuna valutazione finora
- Maxillary SinusDocumento67 pagineMaxillary SinusDR. NEETI TATIYANessuna valutazione finora
- Bab Ii AnjDocumento13 pagineBab Ii Anjteguh fikriNessuna valutazione finora
- OHNS--Otolaryngology; Head and Neck surgery: pocket field guideDa EverandOHNS--Otolaryngology; Head and Neck surgery: pocket field guideNessuna valutazione finora
- Oral Medicine & Pathology from A-ZDa EverandOral Medicine & Pathology from A-ZValutazione: 5 su 5 stelle5/5 (9)
- MaxSinus Lecture 2Documento32 pagineMaxSinus Lecture 2Shajid MaruthoraNessuna valutazione finora
- NDBE Physiology ReviewDocumento104 pagineNDBE Physiology Reviewdaw022100% (2)
- Oral Histology CompendiumDocumento197 pagineOral Histology Compendiumdaw022Nessuna valutazione finora
- Mandibular Nerve Block (Other Techniques)Documento24 pagineMandibular Nerve Block (Other Techniques)daw022100% (2)
- Maxillary Anesthesia - 2Documento35 pagineMaxillary Anesthesia - 2daw022Nessuna valutazione finora
- Middle Superior Alveolar Nerve BlockDocumento39 pagineMiddle Superior Alveolar Nerve Blockdaw022Nessuna valutazione finora
- Anestezia PalatuluiDocumento24 pagineAnestezia PalatuluiVavi NichimisNessuna valutazione finora
- Maxillary Anesthesia - 1Documento12 pagineMaxillary Anesthesia - 1daw022Nessuna valutazione finora
- Lecture 2 Introduction & General Features of Nervous SystemDocumento36 pagineLecture 2 Introduction & General Features of Nervous Systemdaw022Nessuna valutazione finora
- Lecture 4 On Sensory Receptors SeptDocumento27 pagineLecture 4 On Sensory Receptors Septdaw022Nessuna valutazione finora
- BRY's Pathology, 1st SemesterDocumento244 pagineBRY's Pathology, 1st Semesterdaw022Nessuna valutazione finora
- Lecture 3 Sensory Tracts & Sensory CortexDocumento27 pagineLecture 3 Sensory Tracts & Sensory Cortexdaw022Nessuna valutazione finora
- Lecture 1 Introduction & General Features of Nervous SystemDocumento28 pagineLecture 1 Introduction & General Features of Nervous Systemdaw022Nessuna valutazione finora
- Mandibular Nerve BlockDocumento23 pagineMandibular Nerve Blockdaw022Nessuna valutazione finora
- BRY's ImmunologyDocumento51 pagineBRY's Immunologydaw022Nessuna valutazione finora
- Anatomy and Embryology of The Pharynx1Documento27 pagineAnatomy and Embryology of The Pharynx1daw022Nessuna valutazione finora
- The Autonomic Nervous SystemDocumento25 pagineThe Autonomic Nervous Systemdaw022100% (1)
- Antiviral 1Documento22 pagineAntiviral 1daw022Nessuna valutazione finora
- Atlas Anatomyof The PharynxDocumento26 pagineAtlas Anatomyof The Pharynxdaw022Nessuna valutazione finora
- New Dental PulpDocumento139 pagineNew Dental Pulpdaw022100% (1)
- Skin - HistologyDocumento30 pagineSkin - Histologydaw022100% (11)
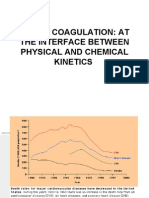
- Blood Coagulation: at The Interface Between Physical and Chemical KineticsDocumento43 pagineBlood Coagulation: at The Interface Between Physical and Chemical Kineticsdaw022Nessuna valutazione finora
- The Central Nervous SystemDocumento35 pagineThe Central Nervous Systemdaw022Nessuna valutazione finora
- Human Physiology ExamsDocumento198 pagineHuman Physiology Examsdaw02250% (4)
- Cranial CavityDocumento17 pagineCranial Cavitydaw022Nessuna valutazione finora
- Moderator: DR - Anil Verma Speaker: Rajeev: Published byDocumento40 pagineModerator: DR - Anil Verma Speaker: Rajeev: Published bydaw022100% (1)
- Loose Connective TissueDocumento25 pagineLoose Connective Tissuedaw022Nessuna valutazione finora
- MusclesDocumento18 pagineMusclesdaw022Nessuna valutazione finora
- Anatomy of The Head & Neck 3 (Mandible)Documento35 pagineAnatomy of The Head & Neck 3 (Mandible)daw022Nessuna valutazione finora
- How Do You Suppose Milken Maintains His Self-Esteem When So Many People Despise Him As A Very Wealthy White Color Criminal?Documento3 pagineHow Do You Suppose Milken Maintains His Self-Esteem When So Many People Despise Him As A Very Wealthy White Color Criminal?Karma GurungNessuna valutazione finora
- A Handbook For Practice Educators and FacilitatorsDocumento144 pagineA Handbook For Practice Educators and FacilitatorsAACCNessuna valutazione finora
- A Project Report On Practice School SubmittedDocumento23 pagineA Project Report On Practice School SubmittedANUJ KUMARNessuna valutazione finora
- Bio ShapeDocumento2 pagineBio ShapeAhmed Hassan AhmedNessuna valutazione finora
- MSRT 0003Documento3 pagineMSRT 0003api-336525339Nessuna valutazione finora
- MSF - Financial - Report - 2021 - FINAL ProvisionalDocumento78 pagineMSF - Financial - Report - 2021 - FINAL ProvisionaldcgfdcNessuna valutazione finora
- Supervisory Relationship GuideDocumento4 pagineSupervisory Relationship GuideremamadhavaNessuna valutazione finora
- Beach Lifeguard Service Implementation GuideDocumento62 pagineBeach Lifeguard Service Implementation GuideAriyadinNessuna valutazione finora
- Abdul Mukmin - Grammar t6Documento3 pagineAbdul Mukmin - Grammar t6QASIM BIN AHMAD MoeNessuna valutazione finora
- Abhishek Kumar Singh - Roll No-01 - TETRA TECH EC CASEDocumento7 pagineAbhishek Kumar Singh - Roll No-01 - TETRA TECH EC CASEscribdabhisheksingh0% (1)
- Drama PTB ScriptDocumento6 pagineDrama PTB ScriptJevialoomsNessuna valutazione finora
- Q-G System Release Notes - OoC 10.29.21Documento13 pagineQ-G System Release Notes - OoC 10.29.21Remik BuczekNessuna valutazione finora
- Does Obesity Cause Type 2 Diabetes MellitusDocumento5 pagineDoes Obesity Cause Type 2 Diabetes Mellitusthebrotherhood2014Nessuna valutazione finora
- ProvidersDocumento110 pagineProvidersmaomao_vt89Nessuna valutazione finora
- CA - LYSOL Disinfecting Wipes (All Sizes, All Scents) - English (Feb 2012) PDFDocumento6 pagineCA - LYSOL Disinfecting Wipes (All Sizes, All Scents) - English (Feb 2012) PDFMartiNessuna valutazione finora
- (Coronavirus) Second Order Effects PDFDocumento17 pagine(Coronavirus) Second Order Effects PDFHimanshu KalraNessuna valutazione finora
- Parson Executive Order 21-10Documento1 paginaParson Executive Order 21-10KevinSeanHeldNessuna valutazione finora
- Common Opposites - Antonyms Vocabulary Word ListDocumento30 pagineCommon Opposites - Antonyms Vocabulary Word ListnixzalNessuna valutazione finora
- Artery Vein CapillaryDocumento1 paginaArtery Vein CapillarynaduniNessuna valutazione finora
- Exploring The STOP-BANG Questionnaire For Obstructive Sleep Apnea Screening in SeniorsDocumento8 pagineExploring The STOP-BANG Questionnaire For Obstructive Sleep Apnea Screening in SeniorsDicka adhitya kamilNessuna valutazione finora
- NIAHO® Accreditation RequirementsDocumento26 pagineNIAHO® Accreditation RequirementsMintesinotNessuna valutazione finora
- Case Study FormatDocumento5 pagineCase Study FormatMICHAEL M. ISIDRONessuna valutazione finora
- Health Plan Financials ExplainedDocumento467 pagineHealth Plan Financials Explainedvidya71v100% (1)
- Personal Fitness Plan to Increase Core StrengthDocumento3 paginePersonal Fitness Plan to Increase Core StrengthJefferson DulayNessuna valutazione finora
- Chapter 2 Rev Sha 812013Documento36 pagineChapter 2 Rev Sha 812013Azimah HamidonNessuna valutazione finora
- Common Medicinal Plants: Tulsi, Aloe Vera & MoreDocumento5 pagineCommon Medicinal Plants: Tulsi, Aloe Vera & MoreAim IndiaNessuna valutazione finora
- Lacey Act Presentation August 2009Documento15 pagineLacey Act Presentation August 2009sisto_madNessuna valutazione finora
- Table BDocumento44 pagineTable Bashwin katareNessuna valutazione finora
- Standigm Raises US $11.5 Million in Series B Round Funding To Advance Its AI-Powered Drug Pipelines Toward License-OutDocumento3 pagineStandigm Raises US $11.5 Million in Series B Round Funding To Advance Its AI-Powered Drug Pipelines Toward License-OutPR.comNessuna valutazione finora
- Psi 2010 44 CateringDocumento5 paginePsi 2010 44 CateringChef ShaneNessuna valutazione finora