Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- KB Strong! - Program For Grinds: Block 2 - Workcapacity/Hypertrophy Block 1 - StrengthDocumento1 paginaKB Strong! - Program For Grinds: Block 2 - Workcapacity/Hypertrophy Block 1 - StrengthmarkNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Greene, Sophia B. Body Image Perceptions, Interpretations and AttitudesDocumento301 pagineGreene, Sophia B. Body Image Perceptions, Interpretations and AttitudesRoxana Coman100% (2)
- Case WS VertigoDocumento24 pagineCase WS VertigoNely KeybumNessuna valutazione finora
- Try Out 10 - 12 - 2016Documento40 pagineTry Out 10 - 12 - 2016AnindyaParamitaMoeljosentonoNessuna valutazione finora
- Try Out 10 - 12 - 2016Documento40 pagineTry Out 10 - 12 - 2016AnindyaParamitaMoeljosentonoNessuna valutazione finora
- Try Out 10 - 12 - 2016Documento40 pagineTry Out 10 - 12 - 2016AnindyaParamitaMoeljosentonoNessuna valutazione finora
- Steinlin Neuropaediatrics 2005Documento8 pagineSteinlin Neuropaediatrics 2005Nely KeybumNessuna valutazione finora
- Saranghyuk Cast: Kim Haejin - Lee Hyuk JaeDocumento1 paginaSaranghyuk Cast: Kim Haejin - Lee Hyuk JaeNely KeybumNessuna valutazione finora
- Steinlin Neuropaediatrics 2005Documento8 pagineSteinlin Neuropaediatrics 2005Nely KeybumNessuna valutazione finora
- Physical and Psychological Correlates of Primary Headache in Young Adulthood: A 26 Year Longitudinal StudyDocumento8 paginePhysical and Psychological Correlates of Primary Headache in Young Adulthood: A 26 Year Longitudinal StudyNely KeybumNessuna valutazione finora
- Journal ReadingDocumento1 paginaJournal ReadingNely KeybumNessuna valutazione finora
- Steinlin Neuropaediatrics 2005Documento8 pagineSteinlin Neuropaediatrics 2005Nely KeybumNessuna valutazione finora
- 1257 FullDocumento7 pagine1257 FullNely KeybumNessuna valutazione finora
- Farmakologi Umum2Documento51 pagineFarmakologi Umum2Nely KeybumNessuna valutazione finora
- Jgo 05 01 036Documento10 pagineJgo 05 01 036Nely KeybumNessuna valutazione finora
- 13 Full-1Documento5 pagine13 Full-1Nely KeybumNessuna valutazione finora
- Jurnal MorbiliDocumento8 pagineJurnal MorbiliNely KeybumNessuna valutazione finora
- JurnalDocumento3 pagineJurnalNely KeybumNessuna valutazione finora
- Jurnal DBDDocumento11 pagineJurnal DBDAkbar_Bako_Akb_153650% (2)
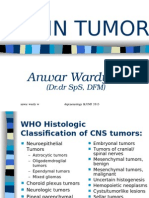
- Brain Tumor: Anwar Wardy WDocumento34 pagineBrain Tumor: Anwar Wardy WNely KeybumNessuna valutazione finora
- PrebiotikDocumento5 paginePrebiotikEssaLoyalLitaLestari100% (1)
- Jgo 05 01 036Documento10 pagineJgo 05 01 036Nely KeybumNessuna valutazione finora
- Kista Duktus CholedocusDocumento11 pagineKista Duktus CholedocusNely KeybumNessuna valutazione finora
- Probiotic Therapy On Children With Allergic RhinitisDocumento4 pagineProbiotic Therapy On Children With Allergic RhinitisSus Retha Mona ArdianiNessuna valutazione finora
- Universal Equation For Estimating Ideal Body Weight and Body Weight at Any BMIDocumento8 pagineUniversal Equation For Estimating Ideal Body Weight and Body Weight at Any BMIcoolboyzoneNessuna valutazione finora
- SL Paper 3: Two Dietary Sources of Vitamin DDocumento28 pagineSL Paper 3: Two Dietary Sources of Vitamin DSugey Constante ToalaNessuna valutazione finora
- Preventing Obesity in ChildrenDocumento5 paginePreventing Obesity in ChildrenWatu WasomeNessuna valutazione finora
- Assignment 03: Computer Programming and Application (ME-214)Documento9 pagineAssignment 03: Computer Programming and Application (ME-214)Asad MirzaNessuna valutazione finora
- Case Study FinalDocumento2 pagineCase Study Finalapi-307578607Nessuna valutazione finora
- Correlation Between Language Development and Motor Skills (Mulé Et Al., 2022)Documento16 pagineCorrelation Between Language Development and Motor Skills (Mulé Et Al., 2022)Alberto I. Cruz FloresNessuna valutazione finora
- Diabetes InformationDocumento171 pagineDiabetes Informationtheia28Nessuna valutazione finora
- Nutritiona L Disorders: Paulette Benjamin-Chin MD Diplomate, Philippine Pediatric SocietyDocumento102 pagineNutritiona L Disorders: Paulette Benjamin-Chin MD Diplomate, Philippine Pediatric SocietygailNessuna valutazione finora
- Đề thi KSCL THPT Chuyên Hạ LongDocumento6 pagineĐề thi KSCL THPT Chuyên Hạ Longant593323Nessuna valutazione finora
- Fast Food Should Be BannedDocumento2 pagineFast Food Should Be BannedHarrinson AlgarinNessuna valutazione finora
- (Publikasi) Farah Diba 1508153938Documento24 pagine(Publikasi) Farah Diba 1508153938faradibaNessuna valutazione finora
- Antropometri AyahDocumento2 pagineAntropometri AyahYAHYA Al-HILALNessuna valutazione finora
- School Form 8 SF8 Learner Basic Health and Nutrition Report Automatic 1Documento16 pagineSchool Form 8 SF8 Learner Basic Health and Nutrition Report Automatic 1Beverly Sison100% (2)
- Studi Prevalensi Risiko Diabetes Melitus Pada Remaja Usia 15-20 Tahun Di Kabupaten SidoarjoDocumento8 pagineStudi Prevalensi Risiko Diabetes Melitus Pada Remaja Usia 15-20 Tahun Di Kabupaten Sidoarjofardiah tilawatiNessuna valutazione finora
- Assignment/ Tugasan - Health and Wellness 1Documento14 pagineAssignment/ Tugasan - Health and Wellness 1Kasturi MahendranNessuna valutazione finora
- Level of Awarenss of Hypertension Among Grade 12 Science Technology Engineering and Mathematics Students of Systems Plus College FoundationDocumento35 pagineLevel of Awarenss of Hypertension Among Grade 12 Science Technology Engineering and Mathematics Students of Systems Plus College FoundationMary Grace MendeNessuna valutazione finora
- Lifetime Physical Fitness and Wellness A Personalized Program 14th Edition Hoeger Solutions Manual 1Documento10 pagineLifetime Physical Fitness and Wellness A Personalized Program 14th Edition Hoeger Solutions Manual 1steve100% (45)
- A First Longitudinal Growth Study of Stature and Weight of The School Children From Jessore District in BangladeshDocumento17 pagineA First Longitudinal Growth Study of Stature and Weight of The School Children From Jessore District in BangladeshIJAR JOURNALNessuna valutazione finora
- Hipertensi GestasionalDocumento12 pagineHipertensi GestasionalFrengki Jeferson DethanNessuna valutazione finora
- Weight Self-Stigma Questionnaire: Steven C. HayesDocumento3 pagineWeight Self-Stigma Questionnaire: Steven C. HayesMitesh HarmalkarNessuna valutazione finora
- Physical Education: Quarter 1Documento5 paginePhysical Education: Quarter 1Lovely BalinoNessuna valutazione finora
- Elevated Blood Pressure: Diagnosis Planning Implementation EvaluatonDocumento3 pagineElevated Blood Pressure: Diagnosis Planning Implementation EvaluatonChloe MorningstarNessuna valutazione finora
- Health Related Fitness Assessment Activity SheetDocumento2 pagineHealth Related Fitness Assessment Activity SheetAlex AlayNessuna valutazione finora
- ESL Brains Should Junk Food Be Taxed TV 7659Documento4 pagineESL Brains Should Junk Food Be Taxed TV 7659Марія ЦонинецьNessuna valutazione finora
- Adhitya Pradana 22010110120064 Bab 8 Kti PDFDocumento28 pagineAdhitya Pradana 22010110120064 Bab 8 Kti PDFsibon M amrilNessuna valutazione finora
- A Clinical Profile of Metabolic Syndrome and Its Determinants Among Police Officers in BaliDocumento5 pagineA Clinical Profile of Metabolic Syndrome and Its Determinants Among Police Officers in BaliDokter FebyanNessuna valutazione finora
- AnthropometryDocumento6 pagineAnthropometrykimwell samsonNessuna valutazione finora
- Carbohydrates PTCDocumento74 pagineCarbohydrates PTCLeonNessuna valutazione finora