Potrebbero piacerti anche
- Case Report Fissure SealantDocumento8 pagineCase Report Fissure SealantrespikNessuna valutazione finora
- Orthodontic Treatment Needs in Adolescents Aged 13-15 Years Using Orthodontic Treatment Needs IndicatorsDocumento7 pagineOrthodontic Treatment Needs in Adolescents Aged 13-15 Years Using Orthodontic Treatment Needs IndicatorsTitis NlgNessuna valutazione finora
- Oral Wound Healing: Cell Biology and Clinical ManagementDa EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaNessuna valutazione finora
- Fixed Orthodontic Appliances: A Practical GuideDa EverandFixed Orthodontic Appliances: A Practical GuideValutazione: 1 su 5 stelle1/5 (1)
- Anopheline Fauna, Hazaribag, JharkhandDocumento4 pagineAnopheline Fauna, Hazaribag, Jharkhandmrazivbu23Nessuna valutazione finora
- Modified Bluegrass Appliance PDFDocumento4 pagineModified Bluegrass Appliance PDFRenieKumalaNessuna valutazione finora
- Pdi Partial EdentulismDocumento67 paginePdi Partial EdentulismAnkeeta ShuklaNessuna valutazione finora
- Developmental DefectsDocumento29 pagineDevelopmental DefectsPrince AhmedNessuna valutazione finora
- Pengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG Denpasar PDFDocumento11 paginePengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG Denpasar PDFZaenuriNessuna valutazione finora
- Fish Bone Analysis of Self-Medication in IndonesiaDocumento6 pagineFish Bone Analysis of Self-Medication in IndonesiaDedy MahendraNessuna valutazione finora
- Pre-Prosthetic Treatment and Tooth PreparationDocumento45 paginePre-Prosthetic Treatment and Tooth PreparationJody JodzNessuna valutazione finora
- Dense Bone Island: Temuan Insidental Pada Radiograf PanoramikDocumento4 pagineDense Bone Island: Temuan Insidental Pada Radiograf PanoramikFransiski HoNessuna valutazione finora
- Coronoplasty 2Documento4 pagineCoronoplasty 2Befalia Aisarahmadani100% (1)
- Splinting 150507152946 Lva1 App6891 PDFDocumento92 pagineSplinting 150507152946 Lva1 App6891 PDFade ismailNessuna valutazione finora
- Space RegainerDocumento7 pagineSpace RegainerdelfNessuna valutazione finora
- JurnalDocumento10 pagineJurnalFranciscoXavierNessuna valutazione finora
- Periodontal Treatment Planning for Patients With Periodontal DiseasesDocumento17 paginePeriodontal Treatment Planning for Patients With Periodontal Diseasesفاطمة فالح ضايف مزعلNessuna valutazione finora
- ADA Caries Risk Assessmento Mayores 6Documento2 pagineADA Caries Risk Assessmento Mayores 6Catalina Cané Muñoz SilvaNessuna valutazione finora
- Modul 6: Kuretase Dan GingivektomiDocumento10 pagineModul 6: Kuretase Dan GingivektomiAGENG RAHMA HIJAHANIS ILMASTITI 1Nessuna valutazione finora
- Fissure TongueDocumento2 pagineFissure Tonguebundahara zoomNessuna valutazione finora
- Decoronation of An Ankylosed Permanent Incisor: Alveolar Ridge Preservation and Rehabilitation by An Implant Supported Porcelain CrownDocumento4 pagineDecoronation of An Ankylosed Permanent Incisor: Alveolar Ridge Preservation and Rehabilitation by An Implant Supported Porcelain CrownJuan Carlos MeloNessuna valutazione finora
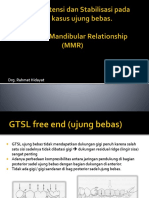
- Dok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRDocumento53 pagineDok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRAditya ZulfikarNessuna valutazione finora
- Clinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFDocumento6 pagineClinical Applications of Biodentine in Pediatric Dentistry A Review Ofliterature 2332 0702 1000179 PDFZita AprilliaNessuna valutazione finora
- AAP Classification of Periodontal DiseasesDocumento16 pagineAAP Classification of Periodontal DiseasesPurwana NasirNessuna valutazione finora
- Curve of SpeeDocumento7 pagineCurve of SpeeKorina CallerosNessuna valutazione finora
- Presentation1 PdiDocumento51 paginePresentation1 PdiAisha samreenNessuna valutazione finora
- Klasifikasi Furcation InvolvementDocumento49 pagineKlasifikasi Furcation InvolvementAnwar KurniawanNessuna valutazione finora
- Classification System For Full EdentulismDocumento4 pagineClassification System For Full EdentulismmandakinimohanNessuna valutazione finora
- Selective grinding review articleDocumento6 pagineSelective grinding review articleNiranjanaNessuna valutazione finora
- Materi Tutor in EnglishDocumento7 pagineMateri Tutor in EnglishDea RachnadewiNessuna valutazione finora
- Kanker MulutDocumento2 pagineKanker MulutHamba AllahNessuna valutazione finora
- Stomatognathic System: - Enosh Steward Nirmalkumar (20) Submitted To Department of OrthodonticsDocumento36 pagineStomatognathic System: - Enosh Steward Nirmalkumar (20) Submitted To Department of OrthodonticsNajeeb UllahNessuna valutazione finora
- 40 130 1 PBDocumento4 pagine40 130 1 PBrinaaa2000Nessuna valutazione finora
- Pharmacological Methods of Behaviour Management PedoDocumento29 paginePharmacological Methods of Behaviour Management PedoFourthMolar.com0% (2)
- Jurnal Reading Bedah MulutDocumento27 pagineJurnal Reading Bedah MulutArismunandar SosiloNessuna valutazione finora
- Frame Denture - Metal Frame BenefitsDocumento8 pagineFrame Denture - Metal Frame BenefitsJennieNessuna valutazione finora
- Abses IntraoralDocumento19 pagineAbses IntraoralTitis LaraswatiNessuna valutazione finora
- 14 - Perawatan Endodontic Gigi Molar Dengan Perforasi BifurkasiDocumento5 pagine14 - Perawatan Endodontic Gigi Molar Dengan Perforasi Bifurkasisarah hanifahNessuna valutazione finora
- Prosthodontic DiagnosisDocumento15 pagineProsthodontic DiagnosisYashpreetsingh Bhatia100% (1)
- 2019 Risk Factors For Caries Development in Primary Sjogren SyndromeDocumento6 pagine2019 Risk Factors For Caries Development in Primary Sjogren SyndromemrsilNessuna valutazione finora
- Majalah IKORTI Desember 2015 PDFDocumento56 pagineMajalah IKORTI Desember 2015 PDFAbdi utomoNessuna valutazione finora
- Extrinsic Stains and Deposits On TeethDocumento9 pagineExtrinsic Stains and Deposits On TeethFredie Jun Onio100% (1)
- Formato Cambra 6 Años en AdelanteDocumento2 pagineFormato Cambra 6 Años en AdelanteSandra GutiérrezNessuna valutazione finora
- Insertion of Complete DentureDocumento6 pagineInsertion of Complete DentureMaulida Dara HarjantiNessuna valutazione finora
- Dentin Hypersensitivity Guide: Causes, Theories, Diagnosis and Treatments /TITLEDocumento29 pagineDentin Hypersensitivity Guide: Causes, Theories, Diagnosis and Treatments /TITLEnovia fiscaNessuna valutazione finora
- Guided Tissue RegenerationDocumento4 pagineGuided Tissue RegenerationNicoleta MarcuNessuna valutazione finora
- SSCDocumento10 pagineSSCYanuar MegaNessuna valutazione finora
- Space Regainers in Pediatric DentistryDocumento6 pagineSpace Regainers in Pediatric DentistryFayiz SäbNessuna valutazione finora
- Preventive Dental MaterialDocumento25 paginePreventive Dental MaterialRischa SafitriNessuna valutazione finora
- FINAL SplintingDocumento46 pagineFINAL SplintingDilmohit SinghNessuna valutazione finora
- Jurnal Pedodonsia ENG 2Documento11 pagineJurnal Pedodonsia ENG 2Uciha Kuku BimaNessuna valutazione finora
- Causes and prevention of ledging and blockages in root canalsDocumento19 pagineCauses and prevention of ledging and blockages in root canalsBunga Erlita RosaliaNessuna valutazione finora
- Daya Hambat Ekstrak Buah Mengkudu (Morinda CitrifoliaDocumento9 pagineDaya Hambat Ekstrak Buah Mengkudu (Morinda CitrifoliaAhmad Willy AntonNessuna valutazione finora
- Cleft Lip and Palate Management: A Comprehensive AtlasDa EverandCleft Lip and Palate Management: A Comprehensive AtlasRicardo D. BennunNessuna valutazione finora
- Understanding Masticatory Function in Unilateral CrossbitesDa EverandUnderstanding Masticatory Function in Unilateral CrossbitesNessuna valutazione finora
- Dentine Hypersensitivity: Developing a Person-centred Approach to Oral HealthDa EverandDentine Hypersensitivity: Developing a Person-centred Approach to Oral HealthNessuna valutazione finora
- Benign Salivary Gland DiseasesDocumento21 pagineBenign Salivary Gland Diseasesmhmdalbdyny764Nessuna valutazione finora
- Dentistry Journal ReadingDocumento28 pagineDentistry Journal ReadingJessica GreenNessuna valutazione finora
- EurJDent92183-8599361 022319Documento6 pagineEurJDent92183-8599361 022319Jessica GreenNessuna valutazione finora
- ROOT Carie A Problem of Growing AgeDocumento3 pagineROOT Carie A Problem of Growing AgeJessica GreenNessuna valutazione finora
- TOEFL Exercise 1Documento12 pagineTOEFL Exercise 1Jessica GreenNessuna valutazione finora
- Effect of Removable Partial Denture On Periodontal HealthDocumento3 pagineEffect of Removable Partial Denture On Periodontal HealthAlex KwokNessuna valutazione finora
- Jaw Lock After TraumaDocumento8 pagineJaw Lock After TraumaJessica GreenNessuna valutazione finora
- NCCLDocumento6 pagineNCCLJessica GreenNessuna valutazione finora
- Necrotizing SialometaplasiaDocumento33 pagineNecrotizing SialometaplasiaJessica GreenNessuna valutazione finora
- METABOLISME PROTEIN+AS - AMINO FKGDocumento59 pagineMETABOLISME PROTEIN+AS - AMINO FKGJessica GreenNessuna valutazione finora
- Vitamin: Nurina TyagitaDocumento42 pagineVitamin: Nurina TyagitaJessica Green100% (1)
- AdjectivesDocumento17 pagineAdjectivesJessica GreenNessuna valutazione finora
- Pasta Gigi (Tooth Paste)Documento18 paginePasta Gigi (Tooth Paste)Jessica GreenNessuna valutazione finora
- DATA WSD Sing AsliDocumento57 pagineDATA WSD Sing AsliJessica GreenNessuna valutazione finora
- Clot, Sánchez, Usán - Ferran, Elisabeth, Elsa - 2nlab - GSFP - P9F5 - Article Científic de Recerca FQDocumento27 pagineClot, Sánchez, Usán - Ferran, Elisabeth, Elsa - 2nlab - GSFP - P9F5 - Article Científic de Recerca FQElisabethNessuna valutazione finora
- Neonatology Cambridge Pocket ClinicianDocumento601 pagineNeonatology Cambridge Pocket Clinicianjuanse1994Nessuna valutazione finora
- Statistical Methods for Calculating Vaccine PD50Documento1 paginaStatistical Methods for Calculating Vaccine PD50Joshua WelchNessuna valutazione finora
- M2 FinalDocumento61 pagineM2 FinalJeranz ColansiNessuna valutazione finora
- Valenzuela City Schools Division Monthly English Test for Grade 8 StudentsDocumento3 pagineValenzuela City Schools Division Monthly English Test for Grade 8 StudentsMiriam Villegas50% (4)
- Briefing Note: Antimicrobial Resistance: An Emerging Water, Sanitation and Hygiene IssueDocumento16 pagineBriefing Note: Antimicrobial Resistance: An Emerging Water, Sanitation and Hygiene IssueBoni MagtibayNessuna valutazione finora
- Module 6 - Laboratory Investigation: Foodborne Disease Outbreak Investigation Team TrainingDocumento44 pagineModule 6 - Laboratory Investigation: Foodborne Disease Outbreak Investigation Team TrainingrepyNessuna valutazione finora
- 6 Managing Complications of IVTDocumento42 pagine6 Managing Complications of IVT4LetterLie31Nessuna valutazione finora
- Week 2. Learning Module Prokaryotic vs. Eukaryotic OrganismDocumento25 pagineWeek 2. Learning Module Prokaryotic vs. Eukaryotic OrganismFezaret Jerome C.Nessuna valutazione finora
- Parasite Infestation TungiasisDocumento14 pagineParasite Infestation TungiasisHadjar Mingfan FlamerNessuna valutazione finora
- Bacterial Meningitis HandoutDocumento7 pagineBacterial Meningitis Handoutapi-648714317Nessuna valutazione finora
- Preparation Outline (Informative Speech)Documento3 paginePreparation Outline (Informative Speech)AmirAircoolNessuna valutazione finora
- NEMATODESDocumento4 pagineNEMATODESAbby VillamuchoNessuna valutazione finora
- Trans Pulmopatho ColoredDocumento8 pagineTrans Pulmopatho Colored2012Nessuna valutazione finora
- PWB 2003Documento19 paginePWB 2003UnnatiNessuna valutazione finora
- RIZAL TECHNOLOGICAL UNIVERSITY NATIONAL SERVICE TRAINING PROGRAM MODULESDocumento9 pagineRIZAL TECHNOLOGICAL UNIVERSITY NATIONAL SERVICE TRAINING PROGRAM MODULESJULIUS CAEZAR CHAVEZNessuna valutazione finora
- Feline Dermatophytosis Treatment RecommendationsDocumento21 pagineFeline Dermatophytosis Treatment RecommendationsFrancisca Thenée SerranoNessuna valutazione finora
- MycotoxinsDocumento20 pagineMycotoxinsibraheem aboyadak100% (1)
- Root Coverage PDFDocumento24 pagineRoot Coverage PDFJason Pak100% (1)
- Vaginal Yeast InfectionDocumento2 pagineVaginal Yeast InfectionwhiteyasminNessuna valutazione finora
- Chronic Rhinitis Types and CausesDocumento14 pagineChronic Rhinitis Types and CausesGunawan AliNessuna valutazione finora
- E. faecalis Endodontic ChallengeDocumento5 pagineE. faecalis Endodontic ChallengeMonica RoopChanderNessuna valutazione finora
- Red Biotechnology ProjectDocumento5 pagineRed Biotechnology ProjectMahendrakumar ManiNessuna valutazione finora
- General characteristics of fungi: Structure, classification, reproduction and diseasesDocumento5 pagineGeneral characteristics of fungi: Structure, classification, reproduction and diseasesDjdjjd SiisusNessuna valutazione finora
- 2.5 - Regional Update: Latin AmericaDocumento10 pagine2.5 - Regional Update: Latin AmericaAqua LakeNessuna valutazione finora
- IPM for Vegetable Pests & DiseasesDocumento53 pagineIPM for Vegetable Pests & DiseasesLeocarl Fabunan Simon RANessuna valutazione finora
- Atis As Mosquito RepellentDocumento5 pagineAtis As Mosquito RepellentAj Gaviola Orito67% (12)
- SCEDermatologySampleQs PDFDocumento21 pagineSCEDermatologySampleQs PDFZoya Annam0% (1)
- Best Practices To Control Late BlightDocumento34 pagineBest Practices To Control Late BlightJorge Luis Alonso G.Nessuna valutazione finora