Potrebbero piacerti anche
- 09 - Monitoring and Complications of Parenteral NutritionDocumento14 pagine09 - Monitoring and Complications of Parenteral Nutritionbocah_britpopNessuna valutazione finora
- 03 - Nutritional Screening and Assessment PDFDocumento8 pagine03 - Nutritional Screening and Assessment PDFbocah_britpop100% (1)
- 17 - Enhanced Recovery PrinciplesDocumento7 pagine17 - Enhanced Recovery Principlesbocah_britpopNessuna valutazione finora
- 17 - Enhanced Recovery PrinciplesDocumento7 pagine17 - Enhanced Recovery Principlesbocah_britpopNessuna valutazione finora
- Materi PerioperatifDocumento11 pagineMateri PerioperatifSyahdat NurkholiqNessuna valutazione finora
- 17 - The Traumatized PatientDocumento7 pagine17 - The Traumatized Patientbocah_britpopNessuna valutazione finora
- 03 - Energy BalanceDocumento8 pagine03 - Energy Balancebocah_britpopNessuna valutazione finora
- 09 - Compounding and Ready-To-use Preparation of PN Pharmaceutical Aspects. Compatibility and Stability Consideration DrugDocumento21 pagine09 - Compounding and Ready-To-use Preparation of PN Pharmaceutical Aspects. Compatibility and Stability Consideration Drugbocah_britpopNessuna valutazione finora
- 08 - Oral and Sip FeedingDocumento11 pagine08 - Oral and Sip Feedingbocah_britpopNessuna valutazione finora
- Interaction of Bone and Vascular Disease in CKDDocumento7 pagineInteraction of Bone and Vascular Disease in CKDbocah_britpopNessuna valutazione finora
- 08 - Oral and Sip FeedingDocumento11 pagine08 - Oral and Sip Feedingbocah_britpopNessuna valutazione finora
- Indications, Contraindications and Monitoring of Enteral NutritionDocumento13 pagineIndications, Contraindications and Monitoring of Enteral Nutritionbocah_britpopNessuna valutazione finora
- 17 - Enhanced Recovery PrinciplesDocumento7 pagine17 - Enhanced Recovery Principlesbocah_britpopNessuna valutazione finora
- 17 - The Traumatized PatientDocumento7 pagine17 - The Traumatized Patientbocah_britpopNessuna valutazione finora
- 08 - Complications and Monitoring of enDocumento7 pagine08 - Complications and Monitoring of enbocah_britpopNessuna valutazione finora
- Weekly ChartDocumento7 pagineWeekly Chartbocah_britpopNessuna valutazione finora
- m84 PDFDocumento14 paginem84 PDFMico Ga Bisa GendutNessuna valutazione finora
- 08 - Techniques of Enteral NutritionDocumento16 pagine08 - Techniques of Enteral Nutritionbocah_britpopNessuna valutazione finora
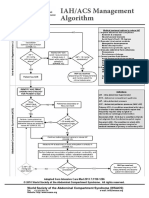
- IAH/ACS Management Algorithm Adapted from Intensive Care MedDocumento1 paginaIAH/ACS Management Algorithm Adapted from Intensive Care Medbocah_britpopNessuna valutazione finora
- 09 - Compounding and Ready-To-use Preparation of PN Pharmaceutical Aspects. Compatibility and Stability Consideration DrugDocumento21 pagine09 - Compounding and Ready-To-use Preparation of PN Pharmaceutical Aspects. Compatibility and Stability Consideration Drugbocah_britpopNessuna valutazione finora
- Materi PerioperatifDocumento11 pagineMateri PerioperatifSyahdat NurkholiqNessuna valutazione finora
- Case Disc RadioDocumento29 pagineCase Disc Radiobocah_britpopNessuna valutazione finora
- Intraabdominal Pressure MonitoringDocumento10 pagineIntraabdominal Pressure Monitoringbocah_britpopNessuna valutazione finora
- Presentation 1Documento2 paginePresentation 1bocah_britpopNessuna valutazione finora
- ACS SabistonDocumento10 pagineACS Sabistonbocah_britpopNessuna valutazione finora
- Interaction of Bone and Vascular Disease in CKDDocumento7 pagineInteraction of Bone and Vascular Disease in CKDbocah_britpopNessuna valutazione finora
- IAH ACS Medical Management 2014Documento1 paginaIAH ACS Medical Management 2014bocah_britpopNessuna valutazione finora
- University of Colorado NICHE Practice Survey SummaryDocumento48 pagineUniversity of Colorado NICHE Practice Survey Summarybocah_britpopNessuna valutazione finora
- Upper Abdominal Pain Case ReportDocumento2 pagineUpper Abdominal Pain Case Reportbocah_britpopNessuna valutazione finora
- HydrocephalusDocumento51 pagineHydrocephalusbocah_britpopNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- HPS STGDocumento33 pagineHPS STGDJGGNessuna valutazione finora
- Billroth ii procedure explainedDocumento2 pagineBillroth ii procedure explainedJasmin MirandaNessuna valutazione finora
- 4 2 - 181 182 PDFDocumento2 pagine4 2 - 181 182 PDFNam LeNessuna valutazione finora
- MCN Test DrillsDocumento20 pagineMCN Test DrillsFamily PlanningNessuna valutazione finora
- QuestionsDocumento26 pagineQuestionsLyka Mae Imbat - PacnisNessuna valutazione finora
- Clinical Gynaecology: Juta - Co.za/pdf/23698Documento3 pagineClinical Gynaecology: Juta - Co.za/pdf/23698Thato MotaungNessuna valutazione finora
- 42 - Circulation and Gas ExchangeDocumento97 pagine42 - Circulation and Gas ExchangeTrisha SantillanNessuna valutazione finora
- Dysphagia Lusoria: A Comprehensive ReviewDocumento6 pagineDysphagia Lusoria: A Comprehensive ReviewDante ChavezNessuna valutazione finora
- Abdominal wall anatomy and common abdominal incisionsDocumento42 pagineAbdominal wall anatomy and common abdominal incisionsSamar AhmadNessuna valutazione finora
- Children's dental health: Retention of teethDocumento4 pagineChildren's dental health: Retention of teethKandiwapaNessuna valutazione finora
- Easy Pharyngeal Anesthesia with Lidocaine LozengesDocumento6 pagineEasy Pharyngeal Anesthesia with Lidocaine LozengespaulaNessuna valutazione finora
- AUTHORIZED HOSPITALS LIST CPRI GOI CGHSDocumento11 pagineAUTHORIZED HOSPITALS LIST CPRI GOI CGHSNaveenkumar PalanisamyNessuna valutazione finora
- Right Flank AbomasopexyDocumento24 pagineRight Flank Abomasopexy7candlesburningNessuna valutazione finora
- Unicompartmental Knee ArthroplastyDocumento10 pagineUnicompartmental Knee Arthroplastycronoss21Nessuna valutazione finora
- Balloon PumpDocumento1 paginaBalloon PumpRaghavendra PrasadNessuna valutazione finora
- Imaging Evaluation of Tracheobronchial InjuriesDocumento14 pagineImaging Evaluation of Tracheobronchial InjuriesSantiago TapiaNessuna valutazione finora
- Colleen J. Rutherford - Differentiating Surgical Instruments (With CDROM) - F. A. Davis Company (First Published March 7th 2005) (2011)Documento211 pagineColleen J. Rutherford - Differentiating Surgical Instruments (With CDROM) - F. A. Davis Company (First Published March 7th 2005) (2011)Amra Fejzic100% (1)
- L1) Oral Cavity, Palate and TongueDocumento39 pagineL1) Oral Cavity, Palate and Tongue3amroooni.a.aNessuna valutazione finora
- Bio Data Name: Prof. Dr. Vinod Kapoor Date/ Place of Birth Educational QualificationsDocumento6 pagineBio Data Name: Prof. Dr. Vinod Kapoor Date/ Place of Birth Educational Qualificationsayub_008Nessuna valutazione finora
- F3 C3 Human Blood Circulatory System ExerciseDocumento3 pagineF3 C3 Human Blood Circulatory System ExerciseCharvini SreeNessuna valutazione finora
- Newborn Capillary Blood CollectionDocumento3 pagineNewborn Capillary Blood CollectionYwagar YwagarNessuna valutazione finora
- Cog Thread LiftDocumento5 pagineCog Thread Liftemilly vidya71% (7)
- Carotid and Vertebral Ultrasonography - Dr. DanielDocumento74 pagineCarotid and Vertebral Ultrasonography - Dr. DanielSuci Rahayu Evasha100% (1)
- GH-ZOLL-Autopulse Quick Case-Instruction ManualDocumento80 pagineGH-ZOLL-Autopulse Quick Case-Instruction ManualjillNessuna valutazione finora
- Medetomidine-Buprenorphine Combo Reduces Isoflurane Needs in CatsDocumento9 pagineMedetomidine-Buprenorphine Combo Reduces Isoflurane Needs in CatsDaniela MartínezNessuna valutazione finora
- Medical Emergency ProcedureDocumento2 pagineMedical Emergency ProcedureAmeena HarisNessuna valutazione finora
- PEMASANGAN ECG 3 LEAD DAN 5 LEADDocumento3 paginePEMASANGAN ECG 3 LEAD DAN 5 LEADPrio Si IyoNessuna valutazione finora
- WelcomeDocumento74 pagineWelcomeSagarRathodNessuna valutazione finora
- Complete IssueDocumento212 pagineComplete IssueAmril MukminNessuna valutazione finora
- V-Gel Cleaning & User GuideDocumento3 pagineV-Gel Cleaning & User GuideInstrulife OostkampNessuna valutazione finora