Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Arabic PronounsDocumento64 pagineArabic Pronounsfatinzalila0% (1)
- Andy Landers - Freeze Zone OffenseDocumento6 pagineAndy Landers - Freeze Zone OffenseWinston Brown100% (1)
- PLSB Comment Not Done - Cable List Summary & Status ReportDocumento26 paginePLSB Comment Not Done - Cable List Summary & Status ReportfatinzalilaNessuna valutazione finora
- Report To PLSB (Issues & Remarks)Documento4 pagineReport To PLSB (Issues & Remarks)fatinzalilaNessuna valutazione finora
- Full Data For Tensile TestDocumento10 pagineFull Data For Tensile TestfatinzalilaNessuna valutazione finora
- Final Viva ZalilaDocumento51 pagineFinal Viva ZalilafatinzalilaNessuna valutazione finora
- Jadual Kelas Sem 1 Tahun 3Documento2 pagineJadual Kelas Sem 1 Tahun 3fatinzalilaNessuna valutazione finora
- CHAPTER 1 Proposal Capstone RWFDocumento7 pagineCHAPTER 1 Proposal Capstone RWFfatinzalilaNessuna valutazione finora
- 01 - Introduction To Computer and Algorithm - PortalDocumento35 pagine01 - Introduction To Computer and Algorithm - PortalfatinzalilaNessuna valutazione finora
- 5 4 18 Obstructions IssuesDocumento8 pagine5 4 18 Obstructions IssuesfatinzalilaNessuna valutazione finora
- Swelling Test ResultDocumento5 pagineSwelling Test ResultfatinzalilaNessuna valutazione finora
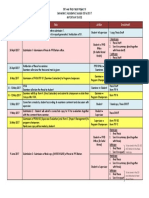
- Important Dates EBT446Documento1 paginaImportant Dates EBT446fatinzalilaNessuna valutazione finora
- Template Data Swelling TestDocumento8 pagineTemplate Data Swelling TestfatinzalilaNessuna valutazione finora
- Advanced Electron Microscopy in The Study of Multimetallic Nanoparticles (Polyol MethodDocumento34 pagineAdvanced Electron Microscopy in The Study of Multimetallic Nanoparticles (Polyol MethodfatinzalilaNessuna valutazione finora
- Slide Viva 1 Proposal RWFDocumento13 pagineSlide Viva 1 Proposal RWFfatinzalilaNessuna valutazione finora
- L08 Metallography PDFDocumento10 pagineL08 Metallography PDFfatinzalilaNessuna valutazione finora
- L09 Distortion Control - PDF - 2Documento4 pagineL09 Distortion Control - PDF - 2fatinzalilaNessuna valutazione finora
- L07 Destructive Test PDFDocumento14 pagineL07 Destructive Test PDFfatinzalila100% (1)
- L11 Production Welding PDFDocumento14 pagineL11 Production Welding PDFfatinzalilaNessuna valutazione finora
- L05 Welding Metallurgy PDFDocumento15 pagineL05 Welding Metallurgy PDFfatinzalilaNessuna valutazione finora
- L04 SmawDocumento16 pagineL04 SmawfatinzalilaNessuna valutazione finora
- Material Selection: Process & Process Selections: Materials Selection and Design EBT 447 SEMESTER I, 2014/2015Documento89 pagineMaterial Selection: Process & Process Selections: Materials Selection and Design EBT 447 SEMESTER I, 2014/2015fatinzalilaNessuna valutazione finora
- L03 Welding Symbols PDFDocumento9 pagineL03 Welding Symbols PDFfatinzalilaNessuna valutazione finora
- Material Selection: Case Studies: Materials Selection and Design EBT 447 SEMESTER II, 2013/2014Documento37 pagineMaterial Selection: Case Studies: Materials Selection and Design EBT 447 SEMESTER II, 2013/2014fatinzalilaNessuna valutazione finora
- Material Selection & DesignDocumento22 pagineMaterial Selection & DesignfatinzalilaNessuna valutazione finora
- Material Selection: Process & Process Selections: Materials Selection and Design EBT 447 SEMESTER I, 2014/2015Documento38 pagineMaterial Selection: Process & Process Selections: Materials Selection and Design EBT 447 SEMESTER I, 2014/2015fatinzalilaNessuna valutazione finora
- CHAPTER 1 Proposal Capstone RWFDocumento7 pagineCHAPTER 1 Proposal Capstone RWFfatinzalilaNessuna valutazione finora
- Materials The Environment: Ebt 447: Materials Selection and DesignDocumento37 pagineMaterials The Environment: Ebt 447: Materials Selection and DesignfatinzalilaNessuna valutazione finora
- Material Selection: Process & Process Selections: Materials Selection and Design EBT 447 SEMESTER I, 2014/2015Documento123 pagineMaterial Selection: Process & Process Selections: Materials Selection and Design EBT 447 SEMESTER I, 2014/2015fatinzalilaNessuna valutazione finora
- Materials Selection FundamentalsDocumento35 pagineMaterials Selection FundamentalsfatinzalilaNessuna valutazione finora
- Full Report Capstone Senior RWFDocumento62 pagineFull Report Capstone Senior RWFfatinzalilaNessuna valutazione finora
- Lecture Notes 1-8Documento39 pagineLecture Notes 1-8Mehdi MohmoodNessuna valutazione finora
- Simple Past Tense The Elves and The Shoemaker Short-Story-Learnenglishteam - ComDocumento1 paginaSimple Past Tense The Elves and The Shoemaker Short-Story-Learnenglishteam - ComgokagokaNessuna valutazione finora
- Umair Mazher ThesisDocumento44 pagineUmair Mazher Thesisumair_mazherNessuna valutazione finora
- I Will Call Upon The Lord - ACYM - NewestDocumento1 paginaI Will Call Upon The Lord - ACYM - NewestGerd SteveNessuna valutazione finora
- The Road To Privatization: TQM and Business Planning: Bennington, Lynne Cummane, JamesDocumento11 pagineThe Road To Privatization: TQM and Business Planning: Bennington, Lynne Cummane, JamesBojan KovacevicNessuna valutazione finora
- ISE I Conversation Task - Rules and RegulationsDocumento3 pagineISE I Conversation Task - Rules and RegulationsElena B. HerreroNessuna valutazione finora
- Vinzenz Hediger, Patrick Vonderau - Films That Work - Industrial Film and The Productivity of Media (Film Culture in Transition) (2009)Documento496 pagineVinzenz Hediger, Patrick Vonderau - Films That Work - Industrial Film and The Productivity of Media (Film Culture in Transition) (2009)Arlindo Rebechi JuniorNessuna valutazione finora
- Word Formation - ExercisesDocumento4 pagineWord Formation - ExercisesAna CiocanNessuna valutazione finora
- Viennas Cafe Louvre in The 1920s and 1930Documento18 pagineViennas Cafe Louvre in The 1920s and 1930Friso HoeneveldNessuna valutazione finora
- Infanrix Hexa RSMKL July 2023Documento37 pagineInfanrix Hexa RSMKL July 2023Bayu KurniawanNessuna valutazione finora
- What Music Really Means To ChildrenDocumento5 pagineWhat Music Really Means To ChildrenMara Sofia ValenteNessuna valutazione finora
- Silvianita - LK 0.1 Modul 2 English For Personal CommunicationDocumento3 pagineSilvianita - LK 0.1 Modul 2 English For Personal CommunicationSilvianita RetnaningtyasNessuna valutazione finora
- DRR Module 4 Detailed Lesson PlanDocumento8 pagineDRR Module 4 Detailed Lesson PlanFe Annalie Sacal100% (2)
- The Forty Nine StepsDocumento312 pagineThe Forty Nine Stepsoldnic67% (3)
- Japanese Tea Cups LessonDocumento3 pagineJapanese Tea Cups Lessonapi-525048974Nessuna valutazione finora
- Philosophical Perspectives Through the AgesDocumento13 paginePhilosophical Perspectives Through the Agesshashankmay18Nessuna valutazione finora
- Hitachi Datasheet Thin Image SnapshotDocumento2 pagineHitachi Datasheet Thin Image Snapshotemail7urangNessuna valutazione finora
- Answer Here:: FAMILY NAME - FIRST NAME - CLASSCODEDocumento4 pagineAnswer Here:: FAMILY NAME - FIRST NAME - CLASSCODEUchayyaNessuna valutazione finora
- Comparative Ethnographies: State and Its MarginsDocumento31 pagineComparative Ethnographies: State and Its MarginsJuan ManuelNessuna valutazione finora
- 2 NDDocumento52 pagine2 NDgal02lautNessuna valutazione finora
- United States Court of Appeals, Sixth CircuitDocumento5 pagineUnited States Court of Appeals, Sixth CircuitScribd Government DocsNessuna valutazione finora
- General Ledger Journal Import ProcessDocumento13 pagineGeneral Ledger Journal Import ProcessMadhavi SinghNessuna valutazione finora
- CHEST 6. Chest Trauma 2022 YismawDocumento61 pagineCHEST 6. Chest Trauma 2022 YismawrobelNessuna valutazione finora
- P7 Summary of ISADocumento76 pagineP7 Summary of ISAAlina Tariq100% (1)
- Health Statement Form Medical Questionnaire (2M Up)Documento1 paginaHealth Statement Form Medical Questionnaire (2M Up)DECA HOMES YAKALNessuna valutazione finora
- Communicative Strategy Powerpoint CO With VideoDocumento20 pagineCommunicative Strategy Powerpoint CO With VideoGlydel Octaviano-GapoNessuna valutazione finora
- Apostles CreedDocumento141 pagineApostles Creedjerome mecca0% (2)
- MF 04Documento21 pagineMF 04Carlos De la CruzNessuna valutazione finora
- Literature ReviewDocumento4 pagineLiterature Reviewapi-549241187Nessuna valutazione finora