Potrebbero piacerti anche
- Cardiovascular Review QuestionsDocumento48 pagineCardiovascular Review Questionsgnikap_deleon0% (1)
- Angina PectorisDocumento8 pagineAngina PectorisJoanne LagusadNessuna valutazione finora
- CARDIOLOGYDocumento15 pagineCARDIOLOGYPatty RomeroNessuna valutazione finora
- Chapter 6 CardiovascularDocumento10 pagineChapter 6 CardiovascularMarie Charmaine100% (1)
- Coronary Artery DiseaseDocumento2 pagineCoronary Artery DiseaseDarell M. BookNessuna valutazione finora
- Cardio 1Documento13 pagineCardio 1TinNessuna valutazione finora
- Critical Care NursingDocumento85 pagineCritical Care NursinganreilegardeNessuna valutazione finora
- MM M M MDocumento20 pagineMM M M MAshok KumarNessuna valutazione finora
- Gastro Intestinal Disorders:: Kawasaki DiseaseDocumento6 pagineGastro Intestinal Disorders:: Kawasaki DiseaseJoanna TaylanNessuna valutazione finora
- Chronic Renal FailureDocumento29 pagineChronic Renal Failuregeorgia.langNessuna valutazione finora
- Patho Test Bank 2021Documento194 paginePatho Test Bank 2021wonyoungg5813100% (1)
- Alterations in VentilationDocumento10 pagineAlterations in VentilationCharisma Pastor100% (1)
- Hide 1 Description 2 Classification 2.1 Chronic Bronchitis 2.2 Emphysema 3 Pathophysiology 4 EpidemiologyDocumento29 pagineHide 1 Description 2 Classification 2.1 Chronic Bronchitis 2.2 Emphysema 3 Pathophysiology 4 EpidemiologyAngie Mandeoya100% (1)
- Assessment of Respiratory Function Chpt.20Documento32 pagineAssessment of Respiratory Function Chpt.20Maricar RosasNessuna valutazione finora
- Medical Surgical Nursing Pre-Test 2 RATIONALEDocumento8 pagineMedical Surgical Nursing Pre-Test 2 RATIONALEBlaine ManiegoNessuna valutazione finora
- Cardiovascular Disease Nursing Diagnosis - Causes - FactsDocumento3 pagineCardiovascular Disease Nursing Diagnosis - Causes - Factsfeirri0% (1)
- Acute Biologic CrisisDocumento6 pagineAcute Biologic CrisismikErlhNessuna valutazione finora
- Cardiovascular: Common Lab Tests For Cardiovascular DisordersDocumento49 pagineCardiovascular: Common Lab Tests For Cardiovascular Disorderssarasmith1988Nessuna valutazione finora
- CardiomyopathyDocumento2 pagineCardiomyopathyBianca SarmientoNessuna valutazione finora
- CardioDocumento7 pagineCardioGerald AndrinNessuna valutazione finora
- Nursing Cardiovascular Physical Examination Made Ridiculously SimpleDocumento17 pagineNursing Cardiovascular Physical Examination Made Ridiculously Simpleedenpearlcastillo100% (2)
- A. Cardiac Failure: Biologic CrisisDocumento11 pagineA. Cardiac Failure: Biologic CrisisJillian CaumbanNessuna valutazione finora
- Neurological Nursing Adult2Documento12 pagineNeurological Nursing Adult2Eug Ulep100% (1)
- Fluid and ElectrolytesDocumento29 pagineFluid and ElectrolytesLinh Tra100% (1)
- Sim Scenario 4Documento31 pagineSim Scenario 4lilchibaby3161Nessuna valutazione finora
- Hema, Onco, Cardiology Review NotesDocumento9 pagineHema, Onco, Cardiology Review Notesjeshema100% (1)
- Pharmacology Bullet ReviewDocumento36 paginePharmacology Bullet ReviewNa Young You100% (1)
- Alteration in OxygenationDocumento8 pagineAlteration in Oxygenationraquel maniegoNessuna valutazione finora
- Print Foundations - Fundamentals of Nursing, Chapter 48 Skin Integrity and Wound Care Flashcards - Easy NotecardsDocumento6 paginePrint Foundations - Fundamentals of Nursing, Chapter 48 Skin Integrity and Wound Care Flashcards - Easy NotecardsMark M. AlipioNessuna valutazione finora
- MEdical Surgical REVEWERDocumento86 pagineMEdical Surgical REVEWERennaedNessuna valutazione finora
- ACE InhibitorsDocumento2 pagineACE InhibitorsJosephine Irena100% (1)
- Testbank OB 1Documento6 pagineTestbank OB 1superrhengcNessuna valutazione finora
- Altered Tissue PerfusionDocumento10 pagineAltered Tissue PerfusionLaurence ZernaNessuna valutazione finora
- 50 Item MedicalDocumento8 pagine50 Item Medicalshark_tale04Nessuna valutazione finora
- Cardiovascular SystemDocumento20 pagineCardiovascular SystemYna MacatangayNessuna valutazione finora
- DigoxinDocumento2 pagineDigoxinNinoska Garcia-Ortiz100% (2)
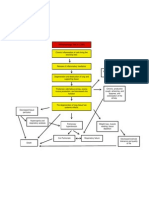
- Patho Tree COPDDocumento1 paginaPatho Tree COPDLaura MitchellNessuna valutazione finora
- Hemorrhagic Cerebro Vascular DiseaseDocumento37 pagineHemorrhagic Cerebro Vascular Diseasejbvaldez100% (1)
- Heart Failure - AhaDocumento77 pagineHeart Failure - AhaChendy Endriansa100% (1)
- Chapter - 001 Health Promotion in Middle-Aged AdultsDocumento10 pagineChapter - 001 Health Promotion in Middle-Aged AdultsTrixie AlvarezNessuna valutazione finora
- Care of Client With Liver and Pancreatic DisorderDocumento28 pagineCare of Client With Liver and Pancreatic Disorderruh820Nessuna valutazione finora
- AUTOIMMUNEDocumento75 pagineAUTOIMMUNEEva Boje-JugadorNessuna valutazione finora
- Acute Kidney Injury (AKI) :: FeaturesDocumento3 pagineAcute Kidney Injury (AKI) :: FeaturesDavid PerezNessuna valutazione finora
- Chapter 3 Fluids and Electrolytes - Acid-Base BalanceDocumento8 pagineChapter 3 Fluids and Electrolytes - Acid-Base BalanceDiony CruzNessuna valutazione finora
- Acid Base Self Study With Practice QuestionsDocumento13 pagineAcid Base Self Study With Practice QuestionsfriendofnurseNessuna valutazione finora
- Sirs & ModsDocumento5 pagineSirs & Modsmarlou agananNessuna valutazione finora
- Hepatobiliary Disorders 2Documento21 pagineHepatobiliary Disorders 2KatrinaJimenezNessuna valutazione finora
- Abg Practice QuizDocumento13 pagineAbg Practice QuizPatty Romero0% (1)
- Case Study Leukemia ScribdDocumento3 pagineCase Study Leukemia ScribdJhoiiceeNessuna valutazione finora
- Drug Overdose and ManagementDocumento9 pagineDrug Overdose and ManagementKoRnflakes100% (1)
- Fluids Electrolytes - Acid-Base BalanceDocumento11 pagineFluids Electrolytes - Acid-Base BalanceJhosita Flora Laroco100% (1)
- Study Guide For Fluid and Electrolyte ImbalancesDocumento5 pagineStudy Guide For Fluid and Electrolyte ImbalancesMandi Goetz HarmonNessuna valutazione finora
- NCM 118Documento14 pagineNCM 118joan bagnateNessuna valutazione finora
- Narrative PathophysiologyDocumento18 pagineNarrative PathophysiologyNica Georgelle Maniego SamonteNessuna valutazione finora
- Nursing Cardiology: Rebound HypertensionDocumento8 pagineNursing Cardiology: Rebound HypertensionVon R SemillaNessuna valutazione finora
- Congestive Heart Failure PDFDocumento9 pagineCongestive Heart Failure PDFSheryl Ann Mae BombalesNessuna valutazione finora
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideDa EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNessuna valutazione finora
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Respiratory Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandRespiratory Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- In Vitro Model For Anti Diabetic AssemntDocumento4 pagineIn Vitro Model For Anti Diabetic AssemntHaleema SultanNessuna valutazione finora
- Polymerase Chain Reaction (PCR)Documento37 paginePolymerase Chain Reaction (PCR)Haleema SultanNessuna valutazione finora
- Animal Rights: "The Worst Sin Towards Our Fellow Creatures Is Not To Hate Them, But ToDocumento22 pagineAnimal Rights: "The Worst Sin Towards Our Fellow Creatures Is Not To Hate Them, But ToHaleema SultanNessuna valutazione finora
- Screening of Anti-Inflammatory DrugsDocumento11 pagineScreening of Anti-Inflammatory DrugsHaleema SultanNessuna valutazione finora
- Screening of Anticonvulsant DrugsDocumento14 pagineScreening of Anticonvulsant DrugsHaleema SultanNessuna valutazione finora
- Interpreting Infrared Spectra Painlessly, Quickly, and CorrectlyDocumento5 pagineInterpreting Infrared Spectra Painlessly, Quickly, and CorrectlyHaleema SultanNessuna valutazione finora
- Institute of Pharmacy Nirma University: Admission Processing Fee (Including Form Fee) : Rs. 1,000/-Web Downloaded FormDocumento5 pagineInstitute of Pharmacy Nirma University: Admission Processing Fee (Including Form Fee) : Rs. 1,000/-Web Downloaded FormHaleema SultanNessuna valutazione finora
- My Project ETHOSOMESDocumento26 pagineMy Project ETHOSOMESHaleema SultanNessuna valutazione finora
- Rigel Uni Pulse Manual v1.3Documento40 pagineRigel Uni Pulse Manual v1.3RandhiMahardhikaNessuna valutazione finora
- Electro-Anatomical Mapping of The HeartDocumento256 pagineElectro-Anatomical Mapping of The HeartHenrique MaiaNessuna valutazione finora
- Circulation: Ms. Jonalyn P. SantosDocumento18 pagineCirculation: Ms. Jonalyn P. SantosHoward John M. RamiterreNessuna valutazione finora
- Nursing Care Plan. HypertensionDocumento2 pagineNursing Care Plan. HypertensionKiara Shanelle Posadas AbrioNessuna valutazione finora
- Ulse Rate Chart: "Heart Attack Warning" Heart Attack Calculate Ideal WeightDocumento2 pagineUlse Rate Chart: "Heart Attack Warning" Heart Attack Calculate Ideal WeightRakesh SinghNessuna valutazione finora
- ECG Interpretations DR RPDocumento109 pagineECG Interpretations DR RPArnis Putri RosyaniNessuna valutazione finora
- The Ehra Book of Intervntional Electrophysiology - OxfordDocumento321 pagineThe Ehra Book of Intervntional Electrophysiology - Oxfordmorris njageNessuna valutazione finora
- 1.cardiac Muscle The Heart As A Pump and Function of The Heart Valves 2022Documento73 pagine1.cardiac Muscle The Heart As A Pump and Function of The Heart Valves 2022Sezanur Taalaibek kyzyNessuna valutazione finora
- ECG TipsDocumento7 pagineECG TipsMar Kristian Vero Lumen100% (1)
- Module 1 Case StudyDocumento5 pagineModule 1 Case Studyapi-564432337100% (1)
- SeminarDocumento34 pagineSeminarMuhammad Faiz Satria WibowoNessuna valutazione finora
- CAD NCP Decreased Cardiac OutputDocumento3 pagineCAD NCP Decreased Cardiac OutputLeizel Apolonio100% (3)
- DefibrillationDocumento13 pagineDefibrillationKristine VedadNessuna valutazione finora
- Itas2010 - Indiantakayasu'S Arteritis Activity ScoreDocumento2 pagineItas2010 - Indiantakayasu'S Arteritis Activity ScoreLp Saikumar DoradlaNessuna valutazione finora
- 2011 ACLS Pretest Annotated Answer KeyDocumento19 pagine2011 ACLS Pretest Annotated Answer KeyMohammed Abdou92% (13)
- 12 Lead EKG 101Documento84 pagine12 Lead EKG 101Clarke KrugmanNessuna valutazione finora
- 2.basic Life SupportDocumento7 pagine2.basic Life SupportNay ThureinNessuna valutazione finora
- PHYSIO 1.06 ECG Interpretation DR - UbinaDocumento7 paginePHYSIO 1.06 ECG Interpretation DR - UbinapachayilstephanoseshintoNessuna valutazione finora
- Acute Cardiac EKG Interpretation - Basics Part 1 - ScriptDocumento2 pagineAcute Cardiac EKG Interpretation - Basics Part 1 - ScriptDarby GravinoNessuna valutazione finora
- Management of Cardiac ArrestDocumento10 pagineManagement of Cardiac ArrestAhmed VelićNessuna valutazione finora
- Principles and Pitfalls in Coronary Vasomotor Function TestingDocumento26 paginePrinciples and Pitfalls in Coronary Vasomotor Function TestingRamón López PalopNessuna valutazione finora
- Shock: Classification, Pathophysiology, and Approach To ManagementDocumento45 pagineShock: Classification, Pathophysiology, and Approach To ManagementClaudia IsabelNessuna valutazione finora
- PacemakerDocumento39 paginePacemakerb7bkroroNessuna valutazione finora
- 3.pemantauan Hemodinamik Non Invasif, Semi Invasif DanDocumento27 pagine3.pemantauan Hemodinamik Non Invasif, Semi Invasif Danikbal rambalinoNessuna valutazione finora
- Age Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting EcgDocumento12 pagineAge Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting EcgRichu UhcirNessuna valutazione finora
- Basic ECG ReadingDocumento41 pagineBasic ECG ReadingBenj100% (3)
- Acls Algorithms 2021 ChecklistDocumento1 paginaAcls Algorithms 2021 ChecklistpepNessuna valutazione finora
- Inotrope: Medical UsesDocumento3 pagineInotrope: Medical UsesCake ManNessuna valutazione finora
- Primedic Defi-BDocumento27 paginePrimedic Defi-BNikolay PenevNessuna valutazione finora
- Basic Concepts of Heart-Lung Interactions During Mechanical VentilationDocumento14 pagineBasic Concepts of Heart-Lung Interactions During Mechanical VentilationanindiawNessuna valutazione finora