Potrebbero piacerti anche
- Blood CultureDocumento22 pagineBlood CulturepawchanNessuna valutazione finora
- How To Treat: Septic ShockDocumento6 pagineHow To Treat: Septic ShockmeeandsoeNessuna valutazione finora
- Incidence and Prevalence PDFDocumento9 pagineIncidence and Prevalence PDFSreya SanilNessuna valutazione finora
- Retinopathy of PrematurityDocumento27 pagineRetinopathy of PrematurityTeoness JoyNessuna valutazione finora
- Standards of Care in Diabetes - 2024Documento9 pagineStandards of Care in Diabetes - 2024josueraulbalandranNessuna valutazione finora
- Secondary ImmunodeficiencyDocumento13 pagineSecondary ImmunodeficiencytanyagargNessuna valutazione finora
- Bladder and Bowel ManagementsDocumento26 pagineBladder and Bowel ManagementsDRKNessuna valutazione finora
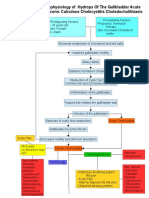
- Pathophysiology of CholecystitisDocumento2 paginePathophysiology of CholecystitisAnonymous gDp7y3Cl82% (22)
- Hodgkin's DiseaseDocumento58 pagineHodgkin's Diseasealibayaty1Nessuna valutazione finora
- Stem Cell TransplantationDocumento13 pagineStem Cell TransplantationMylls MondejarNessuna valutazione finora
- Nosocomial Infections: Dr. Tjatur Winarsanto SPPD RST Ciremai CirebonDocumento48 pagineNosocomial Infections: Dr. Tjatur Winarsanto SPPD RST Ciremai CirebonNovita Trilianty MagdalenaNessuna valutazione finora
- Normal Values - CBCDocumento4 pagineNormal Values - CBCMohammad Salah D. MacapantonNessuna valutazione finora
- Management of Tuberculosis: A guide for clinicians (eBook edition)Da EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Nessuna valutazione finora
- Acute Lymphocytic Leukemia: A Case Presentation by Nollen LaquianDocumento43 pagineAcute Lymphocytic Leukemia: A Case Presentation by Nollen LaquianMonica MoralesNessuna valutazione finora
- Bone Marrow TransplantDocumento8 pagineBone Marrow TransplantPSRI hospitalNessuna valutazione finora
- Pancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandPancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Collection of SpecimenDocumento35 pagineCollection of SpecimenRona Palomo100% (1)
- Case Study - HivDocumento10 pagineCase Study - HivJoycee BurtanogNessuna valutazione finora
- CholangitisDocumento15 pagineCholangitisFaye TanNessuna valutazione finora
- Dimension of Development: Health Awareness: Nstp-Cwts Chapter 6Documento8 pagineDimension of Development: Health Awareness: Nstp-Cwts Chapter 6Rika Mae100% (3)
- Transfusion Reaction and Coombs Test: Moderator:-Dr Sanjay Agrwal Presenter: - DR Pratima Singh PG Jr-1Documento33 pagineTransfusion Reaction and Coombs Test: Moderator:-Dr Sanjay Agrwal Presenter: - DR Pratima Singh PG Jr-1UmikaguptaNessuna valutazione finora
- Pathophysiology Septic ShockDocumento26 paginePathophysiology Septic ShockTinea Sycillia100% (1)
- Brain InfectionDocumento61 pagineBrain Infectionmanisha paikarayNessuna valutazione finora
- Hematologic SystemDocumento81 pagineHematologic Systemseigelystic100% (23)
- Transfusion Medicine All by Manno 2002Documento23 pagineTransfusion Medicine All by Manno 2002we445Nessuna valutazione finora
- Week1 - Intro-Infectious Disease EpidemiologyDocumento42 pagineWeek1 - Intro-Infectious Disease EpidemiologyLee da Don100% (1)
- Acinetobacter BaumanniiDocumento53 pagineAcinetobacter BaumanniiLaboratorium BorromeusNessuna valutazione finora
- MDRO PPT MarcDocumento24 pagineMDRO PPT MarcMarc Andrew100% (1)
- Final Exam 2013 Sample Epidemiology of Infectious DiseasesDocumento7 pagineFinal Exam 2013 Sample Epidemiology of Infectious DiseasesIsha Bhatt100% (1)
- Blood Transfusion Guidelines PDFDocumento21 pagineBlood Transfusion Guidelines PDFEmhemed Amer Tabib100% (2)
- Clostridium DifficileDocumento52 pagineClostridium DifficileAndrés Menéndez RojasNessuna valutazione finora
- Safe Handling Chemotherapy DrugsDocumento62 pagineSafe Handling Chemotherapy DrugsKaterina Georgiadi KalogianniNessuna valutazione finora
- Hanson Infectious Diseases - Anamneza I StatusDocumento33 pagineHanson Infectious Diseases - Anamneza I StatusSilvia KesegNessuna valutazione finora
- Group 1 Apolonio, Leizel, R. Corpuz Rolyn Mañalac Joelle Anne Señeres Loui AnneDocumento33 pagineGroup 1 Apolonio, Leizel, R. Corpuz Rolyn Mañalac Joelle Anne Señeres Loui AnneLeizel ApolonioNessuna valutazione finora
- Laboratory Hematology PracticeDa EverandLaboratory Hematology PracticeKandice Kottke-MarchantValutazione: 5 su 5 stelle5/5 (1)
- Nosocomial Infections - Dr. LindaDocumento30 pagineNosocomial Infections - Dr. LindaGeorge C. KasondaNessuna valutazione finora
- Haemophilus SPPDocumento109 pagineHaemophilus SPPJamie CañebaNessuna valutazione finora
- Nosocomial InfectionDocumento26 pagineNosocomial InfectionAhmad MohamedNessuna valutazione finora
- Concepts of Infection ControlDocumento61 pagineConcepts of Infection Controltummalapalli venkateswara rao100% (1)
- Nosocomial InfectionDocumento13 pagineNosocomial InfectionwabalyNessuna valutazione finora
- Acinetobacter BaumanniiDocumento12 pagineAcinetobacter BaumanniiGIST (Gujarat Institute of Science & Technology)Nessuna valutazione finora
- Problems in Bone Marrow PathologyDocumento29 pagineProblems in Bone Marrow PathologymaurocznNessuna valutazione finora
- Cep Halo SporinsDocumento19 pagineCep Halo SporinsStarlet Rhonadez Bito-onon OrielNessuna valutazione finora
- Blood Transfusion - Indications, Administration and Adverse Reactions PDFDocumento9 pagineBlood Transfusion - Indications, Administration and Adverse Reactions PDFStacey WoodsNessuna valutazione finora
- Viral Hepatitis PDFDocumento4 pagineViral Hepatitis PDFNina BracyNessuna valutazione finora
- Ethics in Healthcare Case ScenariosDocumento1 paginaEthics in Healthcare Case ScenariosA CNessuna valutazione finora
- Systemic Lupus Erythematosus (SLE)Documento39 pagineSystemic Lupus Erythematosus (SLE)Nadya SabrinaNessuna valutazione finora
- Leukemia (Partly)Documento9 pagineLeukemia (Partly)rukipatNessuna valutazione finora
- WHO Guidline On Development of Haemovigilance SystemDocumento19 pagineWHO Guidline On Development of Haemovigilance SystemRustiannaTumanggorNessuna valutazione finora
- Complications of CABGDocumento38 pagineComplications of CABGpriyathasanNessuna valutazione finora
- Tumor MarkersDocumento14 pagineTumor MarkersPatrick LizarondoNessuna valutazione finora
- Status Asthmaticus: Triwahju AstutiDocumento41 pagineStatus Asthmaticus: Triwahju AstutirianiNessuna valutazione finora
- In The Clinic - Acute PancreatitisDocumento16 pagineIn The Clinic - Acute PancreatitisSurapon Nochaiwong100% (1)
- Acute Lymphoid LeukemiaDocumento41 pagineAcute Lymphoid Leukemiaummi ulfahNessuna valutazione finora
- Febrile Neutropenia: Nontapak ThiangpakDocumento53 pagineFebrile Neutropenia: Nontapak ThiangpakRapid MedicineNessuna valutazione finora
- Pharmacology of The GITDocumento31 paginePharmacology of The GITmarviecute22Nessuna valutazione finora
- Questions For OSCE Exam - Model AnswersDocumento9 pagineQuestions For OSCE Exam - Model AnswersFarah FarahNessuna valutazione finora
- Oncologic EmergenciesDocumento32 pagineOncologic EmergenciesColleen BernilNessuna valutazione finora
- 12 Lower Female Genital Tract InfectionsDocumento42 pagine12 Lower Female Genital Tract InfectionsAwal Sher khanNessuna valutazione finora
- BacteriaDocumento168 pagineBacteriadenekeNessuna valutazione finora
- Blood Cell CountDocumento27 pagineBlood Cell CountDiane-Richie PezLoNessuna valutazione finora
- Culture and IdentificationDocumento4 pagineCulture and IdentificationDewa Denis100% (1)
- Cancer Risk FactorsDocumento44 pagineCancer Risk FactorsSalomo Galih NugrohoNessuna valutazione finora
- Guideline Antibiotic RationalDocumento35 pagineGuideline Antibiotic RationalIstianah EsNessuna valutazione finora
- Safe Blood: Purifying the Nations Blood Supply in the Age of ADa EverandSafe Blood: Purifying the Nations Blood Supply in the Age of ANessuna valutazione finora
- PBHL 625 Longitudinal Data Analysis - Fall 2014Documento3 paginePBHL 625 Longitudinal Data Analysis - Fall 2014Isha BhattNessuna valutazione finora
- Sasrtf For LDADocumento6 pagineSasrtf For LDAIsha BhattNessuna valutazione finora
- 02 ImmunizationDocumento4 pagine02 ImmunizationIsha BhattNessuna valutazione finora
- Contoh Soal Uji Kompetensi Keperawatan KomunitasDocumento39 pagineContoh Soal Uji Kompetensi Keperawatan KomunitasUmairohSetengahTiga67% (3)
- Doh DC 2018-0142Documento2 pagineDoh DC 2018-0142vanceNessuna valutazione finora
- Epidemiology Computational ModelsDocumento16 pagineEpidemiology Computational ModelsIbrahim Jynx FalamaNessuna valutazione finora
- Typhoid Fever: Presented by Sharlin MacalintalDocumento18 pagineTyphoid Fever: Presented by Sharlin MacalintalPaul JacksonNessuna valutazione finora
- TestresultDocumento2 pagineTestresultaasirNessuna valutazione finora
- New First Aid With BLS PresentationDocumento115 pagineNew First Aid With BLS PresentationSheena Mae MahinayNessuna valutazione finora
- Epidemiology AssignmentDocumento12 pagineEpidemiology AssignmentSagar ParajuliNessuna valutazione finora
- Chickenpox (Varicella) : Questions and Answers: Information About The Disease and VaccinesDocumento3 pagineChickenpox (Varicella) : Questions and Answers: Information About The Disease and VaccinesKailash NagarNessuna valutazione finora
- Innocent ResearchDocumento31 pagineInnocent ResearchInnocent njogopaNessuna valutazione finora
- Lung CarcinomaDocumento29 pagineLung Carcinomavinoedhnaidu_rajagopalNessuna valutazione finora
- Nutrients 11 00655Documento20 pagineNutrients 11 00655Ibtidau NiamilahNessuna valutazione finora
- Pengembangan Aplikasi Monitoring Penyakit Hipertensi Dan Diabetes Mellitus TerintegrasiDocumento15 paginePengembangan Aplikasi Monitoring Penyakit Hipertensi Dan Diabetes Mellitus TerintegrasiberiNessuna valutazione finora
- Anaerobic Bacteria QuizletDocumento6 pagineAnaerobic Bacteria QuizletReca Marie FRIASNessuna valutazione finora
- Evaluation of Microscopic HematuriaDocumento15 pagineEvaluation of Microscopic HematuriaAndi SusiloNessuna valutazione finora
- Framingham Heart Study PDFDocumento5 pagineFramingham Heart Study PDFCarlos Fernando RíosNessuna valutazione finora
- Dik Sakit PDFDocumento117 pagineDik Sakit PDFrisky royatinNessuna valutazione finora
- Sba #4 - STDSDocumento6 pagineSba #4 - STDSlucyNessuna valutazione finora
- NCP Knowledge DeficitDocumento2 pagineNCP Knowledge DeficitRainier IbarretaNessuna valutazione finora
- 5 Pengkajian Awal Medis & Keperawatan (RI)Documento2 pagine5 Pengkajian Awal Medis & Keperawatan (RI)nurkholilaNessuna valutazione finora
- Vaccine and ImmunityDocumento32 pagineVaccine and ImmunityAlona SangamNessuna valutazione finora
- Internal Medicine II II MidtermDocumento11 pagineInternal Medicine II II MidtermJerin XavierNessuna valutazione finora
- Tut 202 2018 S1Documento23 pagineTut 202 2018 S1Feroza AngamiaNessuna valutazione finora
- What Is DracunculiasisDocumento1 paginaWhat Is DracunculiasisSiti SyahirahNessuna valutazione finora
- CuesDocumento8 pagineCuesFloyd SevillaNessuna valutazione finora