Potrebbero piacerti anche
- Sics Steps: Divisi Katarak Dan Bedah Refraktif Rumah Sakit Mata Bali MandaraDocumento74 pagineSics Steps: Divisi Katarak Dan Bedah Refraktif Rumah Sakit Mata Bali MandaraPande GustianaNessuna valutazione finora
- Teknik Operasi KatarakDocumento33 pagineTeknik Operasi KatarakD'Mhan MbozoNessuna valutazione finora
- SICS Cataract Surgery Complications PreventionDocumento9 pagineSICS Cataract Surgery Complications Preventioninna_luv_u9006Nessuna valutazione finora
- PhacoemulsificationDocumento54 paginePhacoemulsificationIshita Kinra100% (1)
- Phco LectureDocumento57 paginePhco Lecturemedhanit anjuloNessuna valutazione finora
- Vitreous Prolapse ManagementDocumento31 pagineVitreous Prolapse ManagementR.m. AndriyanNessuna valutazione finora
- Basic VitrectomyDocumento24 pagineBasic Vitrectomykomitemedik.rsudsdaNessuna valutazione finora
- Nov 20: Journey in Neuroendoscopy: SinghDocumento21 pagineNov 20: Journey in Neuroendoscopy: SinghAtharv SinghNessuna valutazione finora
- Eye ProblemsDocumento25 pagineEye ProblemsHikmat UllahNessuna valutazione finora
- Cataract Surgery: Past-Present-FutureDocumento44 pagineCataract Surgery: Past-Present-FutureNica Lopez FernandezNessuna valutazione finora
- CricothyroidotomyDocumento41 pagineCricothyroidotomyNur SusiawantyNessuna valutazione finora
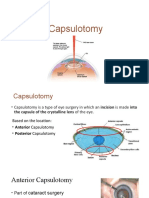
- CapsulotomyDocumento15 pagineCapsulotomyAdrian PearlNessuna valutazione finora
- Trabeculectomy Procedure for Lowering Eye PressureDocumento42 pagineTrabeculectomy Procedure for Lowering Eye PressureAnita Zhang100% (1)
- Surgical Management of Senile CataractDocumento39 pagineSurgical Management of Senile CataractKarthik ChellaNessuna valutazione finora
- Spineinstrumentation 220325073013Documento98 pagineSpineinstrumentation 220325073013Anwer YahyaNessuna valutazione finora
- Permanent Tunnel CatheterDocumento52 paginePermanent Tunnel CatheterJanice MuliadiNessuna valutazione finora
- ENT QuestionsDocumento24 pagineENT QuestionsVijay BabuNessuna valutazione finora
- 3266 Small Incision Cataract Booklet Low ResDocumento37 pagine3266 Small Incision Cataract Booklet Low ResDiana NovacNessuna valutazione finora
- Why When and HowDocumento11 pagineWhy When and Howamrit koiralaNessuna valutazione finora
- Oculofacial Plastic and Orbital SurgeryDocumento14 pagineOculofacial Plastic and Orbital SurgeryTakwinNessuna valutazione finora
- Basics of Microvascular SurgeryDocumento33 pagineBasics of Microvascular SurgeryPratikshya KothiaNessuna valutazione finora
- Gingivectomy & CurettageDocumento55 pagineGingivectomy & CurettageRajani GedelaNessuna valutazione finora
- Eye ProsthesesDocumento75 pagineEye ProsthesesNiharika SabharwalNessuna valutazione finora
- The Flap Technique for Pocket TherapyDocumento34 pagineThe Flap Technique for Pocket TherapyNia Lieanto0% (1)
- Surgicalairwaytechniques 180526060828 PDFDocumento72 pagineSurgicalairwaytechniques 180526060828 PDFWael ShamyNessuna valutazione finora
- ICP MonitoringDocumento2 pagineICP MonitoringMandyAoNessuna valutazione finora
- ACCESS CAVITY PREPARATION GUIDELINESDocumento35 pagineACCESS CAVITY PREPARATION GUIDELINESShaheen Aboobacker Reniya ShaheenNessuna valutazione finora
- Small Incision Cataract Surgery: Kumar Vaibhav 3 Year MD Ophthalmology Resident Bpklcos, TuthDocumento67 pagineSmall Incision Cataract Surgery: Kumar Vaibhav 3 Year MD Ophthalmology Resident Bpklcos, TuthSriniwasNessuna valutazione finora
- Surgery of The EyeDocumento3 pagineSurgery of The Eyehonovezaann.a.campita.ctucvmNessuna valutazione finora
- Insertion and Operation of IABP-1Documento10 pagineInsertion and Operation of IABP-1Atia KiranNessuna valutazione finora
- ISMT 12 - Day 519 - Vito - Surgery For Epidural and Subdural HematomasDocumento24 pagineISMT 12 - Day 519 - Vito - Surgery For Epidural and Subdural HematomasVito MasagusNessuna valutazione finora
- Neck DissectionDocumento45 pagineNeck DissectionAbel AbrahamNessuna valutazione finora
- 3.2. ECMO Cannulation and PitfallDocumento85 pagine3.2. ECMO Cannulation and PitfallEko SarwowibowoNessuna valutazione finora
- Temporal Bone Dissection ManualDocumento15 pagineTemporal Bone Dissection Manualabhi2537100% (1)
- Small Incision Cataract SurgeryDocumento8 pagineSmall Incision Cataract Surgerykefi998100% (3)
- Cornea Outpatient Procedures GuideDocumento59 pagineCornea Outpatient Procedures GuideSana ParveenNessuna valutazione finora
- Harvesting SVGDocumento26 pagineHarvesting SVGSamuel Hotma Rotua Sinaga100% (1)
- Steps Cataract ExtractionDocumento9 pagineSteps Cataract ExtractionJustin John NavarroNessuna valutazione finora
- Managing Full-Thickness Eyelid Lacerations With Canalicular InvolvementDocumento30 pagineManaging Full-Thickness Eyelid Lacerations With Canalicular InvolvementLingula AurikulaNessuna valutazione finora
- Capsulorhexis in Phacoemulsification SurgeryDocumento24 pagineCapsulorhexis in Phacoemulsification SurgeryPawan JarwalNessuna valutazione finora
- Nipple Reconstruction FINALDocumento39 pagineNipple Reconstruction FINALBarath Kumar SinghNessuna valutazione finora
- Correcting Astigmatism with Toric IOLsDocumento28 pagineCorrecting Astigmatism with Toric IOLsArif MohammadNessuna valutazione finora
- Eye and Ocular AdnexaDocumento19 pagineEye and Ocular AdnexaANJALI RAWATNessuna valutazione finora
- Endoscopy Layth Mahmoud HussainDocumento15 pagineEndoscopy Layth Mahmoud Hussainnoor deenNessuna valutazione finora
- Rhinoplasty 이홍경Documento53 pagineRhinoplasty 이홍경entgo8282Nessuna valutazione finora
- Lens Anterior Capsule Opening ProceduresDocumento15 pagineLens Anterior Capsule Opening ProceduresDr Sudhir SinghNessuna valutazione finora
- Cataract Coach BookDocumento62 pagineCataract Coach Bookravian8bNessuna valutazione finora
- 07 Special E (Fako)Documento21 pagine07 Special E (Fako)srihandayaniakbarNessuna valutazione finora
- Anatomy of Angle of Anterior ChamberDocumento67 pagineAnatomy of Angle of Anterior ChamberRahnaNessuna valutazione finora
- Aqueous Drainage Devices: Major ReviewDocumento3 pagineAqueous Drainage Devices: Major ReviewAhmad Angga LuthfiNessuna valutazione finora
- Dokumen - Tips RirsDocumento98 pagineDokumen - Tips RirsBela RonaldoeNessuna valutazione finora
- Extracapsular Cataract Extraction (Ecce)Documento9 pagineExtracapsular Cataract Extraction (Ecce)Nica Lopez FernandezNessuna valutazione finora
- 05 EcceDocumento9 pagine05 EccebebibebihoNessuna valutazione finora
- Subtotal Petrosectomy Procedure GuideDocumento9 pagineSubtotal Petrosectomy Procedure GuideKhzNessuna valutazione finora
- Periodontal Flaps: DR Sadia Tabassum Asst Prof Optv Dent JMDCDocumento74 paginePeriodontal Flaps: DR Sadia Tabassum Asst Prof Optv Dent JMDCayesha100% (1)
- Posterior Polar Cataract Management: My Approach: 2022, #1Da EverandPosterior Polar Cataract Management: My Approach: 2022, #1Nessuna valutazione finora
- White Intumescent Cataract Management: My Approach: 2022, #1Da EverandWhite Intumescent Cataract Management: My Approach: 2022, #1Nessuna valutazione finora
- Cataract And Small Pupil Management Manual Techniques: 2022, #1Da EverandCataract And Small Pupil Management Manual Techniques: 2022, #1Nessuna valutazione finora
- Daftar PustakaDocumento1 paginaDaftar PustakaCok Krishna D. PemayunNessuna valutazione finora
- Untitled 1Documento1 paginaUntitled 1Cok Krishna D. PemayunNessuna valutazione finora
- Untitled 1Documento1 paginaUntitled 1Cok Krishna D. PemayunNessuna valutazione finora
- Untitled 1Documento1 paginaUntitled 1Cok Krishna D. PemayunNessuna valutazione finora
- Toplabs Catalog 1Documento16 pagineToplabs Catalog 1esteriplasNessuna valutazione finora
- IJRASS Journal Thomson ReuterDocumento3 pagineIJRASS Journal Thomson ReuterIrfanMarwanzaNessuna valutazione finora
- "Drug Induced Erythema Multiforme" - A ReviewDocumento7 pagine"Drug Induced Erythema Multiforme" - A ReviewNauroh NaurohNessuna valutazione finora
- Pissn 2085-9481 Eissn 2597-999X Jurnal Biomedik. 2020 12 (1) :31-37Documento7 paginePissn 2085-9481 Eissn 2597-999X Jurnal Biomedik. 2020 12 (1) :31-37Kiky HaryantariNessuna valutazione finora
- Prentice9e Im Chap19Documento6 paginePrentice9e Im Chap19api-2813400240% (1)
- Ujian Semester Gasal Bing Kelas Xii Ipa-1,2 Paket 2Documento15 pagineUjian Semester Gasal Bing Kelas Xii Ipa-1,2 Paket 2Richard sutantoNessuna valutazione finora
- Showa University Introduces Dental Patient RobotDocumento4 pagineShowa University Introduces Dental Patient RobotDent YomarajNessuna valutazione finora
- Nicu Must KnowsDocumento7 pagineNicu Must KnowsCyfern100% (2)
- Oral and Maxillofacial PathologyDocumento79 pagineOral and Maxillofacial PathologyMai AnhNessuna valutazione finora
- Medical ProformaDocumento6 pagineMedical ProformaShahaan ZulfiqarNessuna valutazione finora
- Malcolm Mills Potion Book Oils PDFDocumento230 pagineMalcolm Mills Potion Book Oils PDFValeria Ambrosio80% (5)
- Circulatory System in 40 CharactersDocumento4 pagineCirculatory System in 40 CharacterssammyNessuna valutazione finora
- Biologi Bordetella PertussisDocumento7 pagineBiologi Bordetella PertussisSetyadinda Putri MalindaNessuna valutazione finora
- Neurological AssessmentDocumento3 pagineNeurological AssessmentGellian Placido100% (3)
- An Tibi OtikDocumento8 pagineAn Tibi OtikMuthi MelatiaraNessuna valutazione finora
- Daftar PustakaDocumento7 pagineDaftar PustakaRahyogkusNessuna valutazione finora
- Barodontalgia 2009Documento6 pagineBarodontalgia 2009Maganti Sai SandeepNessuna valutazione finora
- Philoderm Professional Peeling GuideDocumento60 paginePhiloderm Professional Peeling GuideNiculae Bogdan Dimitrie100% (1)
- Chapter 9 - Middle - and Long-Latency Auditory Evoked PotentialsDocumento23 pagineChapter 9 - Middle - and Long-Latency Auditory Evoked PotentialsCaio LeônidasNessuna valutazione finora
- Master LBM 1 IntanDocumento19 pagineMaster LBM 1 IntanCyntia AndrinaNessuna valutazione finora
- MAPEH 7 3rd Quarter ExamDocumento5 pagineMAPEH 7 3rd Quarter Examlaarni malata100% (1)
- Stok Opname November 17Documento12 pagineStok Opname November 17farid akbarNessuna valutazione finora
- CHN Rle ReviewerDocumento10 pagineCHN Rle ReviewerKenneth Fe AgronNessuna valutazione finora
- Safety Blood Bank By-Dr - Mohamed Barouni 222Documento31 pagineSafety Blood Bank By-Dr - Mohamed Barouni 222Hannan AliNessuna valutazione finora
- Citrus Fruit As A Bacterial Hand SanitizerDocumento14 pagineCitrus Fruit As A Bacterial Hand SanitizerPrecious Nicole100% (1)
- Palliative Prognostic ScoreDocumento2 paginePalliative Prognostic ScoreAnastasia Yovita SariNessuna valutazione finora
- Respiratory Diseases: Communicable Diseases of Tuberculosis and PneumoniaDocumento37 pagineRespiratory Diseases: Communicable Diseases of Tuberculosis and PneumoniaCharlz ZipaganNessuna valutazione finora
- Writing Subtest For NursingDocumento4 pagineWriting Subtest For NursingDC BranchNessuna valutazione finora
- Activity Design Nutrition Month 2019Documento6 pagineActivity Design Nutrition Month 2019Ruth Catibag JavellanaNessuna valutazione finora
- Betadine Solution 10 Percent 2007-1Documento8 pagineBetadine Solution 10 Percent 2007-1Jason SmithNessuna valutazione finora