Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Skilled Nursing Documentation Guide PDFDocumento81 pagineSkilled Nursing Documentation Guide PDFcharitoaveNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Respiratory Study Guide 3Documento5 pagineRespiratory Study Guide 3charitoaveNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Hesi FundamentalsDocumento14 pagineHesi Fundamentalscharitoave90% (20)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Neuro3: Study Online atDocumento3 pagineNeuro3: Study Online atcharitoaveNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Mneumonics To PrintDocumento22 pagineMneumonics To Printcharitoave100% (2)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Acute POC For DiarrheaDocumento2 pagineAcute POC For DiarrheacharitoaveNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- PharmDocumento1 paginaPharmcharitoaveNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Meds Sideeffects1Documento7 pagineMeds Sideeffects1Alejandro Bocanegra OsunaNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Live ReviewDocumento1 paginaLive ReviewcharitoaveNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Lab ValuesDocumento1 paginaLab ValueszbestgurlNessuna valutazione finora
- MedsDocumento8 pagineMedscharitoaveNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Meds Sideeffects1Documento7 pagineMeds Sideeffects1Alejandro Bocanegra OsunaNessuna valutazione finora
- All Conditions NclexDocumento7 pagineAll Conditions NclexcharitoaveNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- ProceduresDocumento6 pagineProcedurescharitoaveNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Endocrine HormonesDocumento3 pagineEndocrine HormonescharitoaveNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Common Meds For NclexDocumento1 paginaCommon Meds For Nclexcharitoave100% (3)
- Saunders Normal ValuesDocumento1 paginaSaunders Normal ValuescharitoaveNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Mneumonics To PrintDocumento22 pagineMneumonics To Printcharitoave100% (2)
- Endocrine DiseasesDocumento6 pagineEndocrine DiseasescharitoaveNessuna valutazione finora
- Nclex Drugs 50Documento4 pagineNclex Drugs 50charitoave100% (2)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Ob 2Documento2 pagineOb 2charitoaveNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Endocrine HormonesDocumento3 pagineEndocrine HormonescharitoaveNessuna valutazione finora
- Endocrine DiseasesDocumento6 pagineEndocrine DiseasescharitoaveNessuna valutazione finora
- Chapter 7 - Stress - TransformationsDocumento21 pagineChapter 7 - Stress - TransformationsroselleNessuna valutazione finora
- Critical Analysis of W.H Auden Poems The PDFDocumento8 pagineCritical Analysis of W.H Auden Poems The PDFMöĤämmĔd äĹ-ŚäÁdï100% (1)
- Islam and Civilization (Analysis Study On The History of Civilization in Islam) Muhammad Hifdil IslamDocumento18 pagineIslam and Civilization (Analysis Study On The History of Civilization in Islam) Muhammad Hifdil IslamLoveth KonniaNessuna valutazione finora
- BIF-V Medium With Preload: DN Value 130000Documento2 pagineBIF-V Medium With Preload: DN Value 130000Robi FirdausNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Child DevelopmentDocumento15 pagineChild Development4AndreeaNessuna valutazione finora
- AS and A Level: ChemistryDocumento11 pagineAS and A Level: ChemistryStingy BieNessuna valutazione finora
- RepaHeel Beeswax-Based Gel For Treating Heel Spurs Has Been Produced in EUDocumento2 pagineRepaHeel Beeswax-Based Gel For Treating Heel Spurs Has Been Produced in EUPR.comNessuna valutazione finora
- Gujral FCMDocumento102 pagineGujral FCMcandiddreamsNessuna valutazione finora
- Las Tech Drafting 3Q WKDocumento13 pagineLas Tech Drafting 3Q WKClemenda TuscanoNessuna valutazione finora
- GSD Puppy Training Essentials PDFDocumento2 pagineGSD Puppy Training Essentials PDFseja saulNessuna valutazione finora
- Iodide and Bromide Ions in Brackish Water, Seawater, and Brines D 3869 - 04Documento12 pagineIodide and Bromide Ions in Brackish Water, Seawater, and Brines D 3869 - 04stevgonNessuna valutazione finora
- Asteroids Prospective EnergyDocumento710 pagineAsteroids Prospective EnergySlavica Otovic100% (1)
- Tips For A Healthy PregnancyDocumento2 pagineTips For A Healthy PregnancyLizaNessuna valutazione finora
- Exam 3 DynamicsDocumento7 pagineExam 3 DynamicsJulioNessuna valutazione finora
- Segmentation of Blood Vessels Using Rule-Based and Machine-Learning-Based Methods: A ReviewDocumento10 pagineSegmentation of Blood Vessels Using Rule-Based and Machine-Learning-Based Methods: A ReviewRainata PutraNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Essential Calculus Skills Practice Workbook With Full SolutionsDocumento528 pagineEssential Calculus Skills Practice Workbook With Full SolutionsGerardo Navarro Sánchez94% (65)
- Notes Transfer of Thermal EnergyDocumento12 pagineNotes Transfer of Thermal Energymahrosh mamoon100% (2)
- GBJ0232 - en GLX 3101 T2Documento43 pagineGBJ0232 - en GLX 3101 T2mnbvqwert100% (2)
- Gondola CalculationDocumento6 pagineGondola CalculationBudi SusantoNessuna valutazione finora
- Carrefour-SA Shopping Center TurkeyDocumento2 pagineCarrefour-SA Shopping Center TurkeyVineet JogalekarNessuna valutazione finora
- DJI F450 Construction Guide WebDocumento21 pagineDJI F450 Construction Guide WebPutu IndrayanaNessuna valutazione finora
- Regression Analysis Random Motors ProjectDocumento22 pagineRegression Analysis Random Motors ProjectPrateek AgrawalNessuna valutazione finora
- Line Differential Protection Red670Documento8 pagineLine Differential Protection Red670igorsfaceNessuna valutazione finora
- Document List - Eni Progetti - Algeria BRN-MLE - 2019-06-10Documento18 pagineDocument List - Eni Progetti - Algeria BRN-MLE - 2019-06-10Naceri Mohamed RedhaNessuna valutazione finora
- Earth Science Essential Learning Competencies 2020Documento5 pagineEarth Science Essential Learning Competencies 2020Charry CervantesNessuna valutazione finora
- Airport Security Post 9-11Documento7 pagineAirport Security Post 9-11lewisNessuna valutazione finora
- Rectifier 5G High Density Embedded Power (3U Power Rack, Three Phase Four Wire) E...Documento4 pagineRectifier 5G High Density Embedded Power (3U Power Rack, Three Phase Four Wire) E...Lintas LtiNessuna valutazione finora
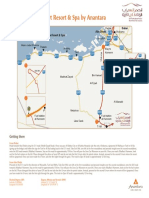
- Qasr Al Sarab Desert Resort Location Map June2012Documento1 paginaQasr Al Sarab Desert Resort Location Map June2012Anant GârgNessuna valutazione finora
- Test 2 Sku3023 A201 QuestionDocumento8 pagineTest 2 Sku3023 A201 QuestionHafiz HafizanNessuna valutazione finora
- Nomenclatura SKFDocumento1 paginaNomenclatura SKFJuan José MeroNessuna valutazione finora
- What to Expect When You’re Expecting (5th Edition)Da EverandWhat to Expect When You’re Expecting (5th Edition)Valutazione: 5 su 5 stelle5/5 (1)
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayDa EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayValutazione: 5 su 5 stelle5/5 (2)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouDa EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNessuna valutazione finora
- ADHD Women: A Holistic Approach To ADHD ManagementDa EverandADHD Women: A Holistic Approach To ADHD ManagementValutazione: 5 su 5 stelle5/5 (4)
- Labor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodDa EverandLabor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodValutazione: 4.5 su 5 stelle4.5/5 (28)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeDa EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeValutazione: 3.5 su 5 stelle3.5/5 (13)