Potrebbero piacerti anche
- Med Surg ATI1Documento97 pagineMed Surg ATI12Ghzchapter88% (17)
- Fluid and Electrolytes for Nursing StudentsDa EverandFluid and Electrolytes for Nursing StudentsValutazione: 5 su 5 stelle5/5 (12)
- Compressive Ati PDFDocumento9 pagineCompressive Ati PDFsarahjaimeeNessuna valutazione finora
- ATI MedSurg BDocumento5 pagineATI MedSurg BHeidi Monsalud100% (6)
- Gi NclexDocumento14 pagineGi NclexYoke W Khoo100% (3)
- Pediatric HESI Review 2016Documento9 paginePediatric HESI Review 2016Brittany78% (9)
- Ati Med SurgDocumento36 pagineAti Med SurgVanessaMUeller94% (17)
- Lewis: Medical-Surgical Nursing, 7th Edition: Comprehensive GlossaryDocumento49 pagineLewis: Medical-Surgical Nursing, 7th Edition: Comprehensive Glossarylani50% (2)
- Med Surge 2 Mod 1 CardiacDocumento13 pagineMed Surge 2 Mod 1 CardiacDirk Buckner100% (2)
- Study Guide Med Surg #1Documento22 pagineStudy Guide Med Surg #1cfunk929Nessuna valutazione finora
- Ati Nclex Review Ob Y6k2c6Documento62 pagineAti Nclex Review Ob Y6k2c6Sunny100% (1)
- Medical Surgical Nursing 7th Edition Ignatavicius Test BankDocumento9 pagineMedical Surgical Nursing 7th Edition Ignatavicius Test Bankqocax0% (1)
- Hurst - Content Review - Cardio (Edit)Documento8 pagineHurst - Content Review - Cardio (Edit)Elaine NorbergNessuna valutazione finora
- Med-Surg HESI Study GuideDocumento13 pagineMed-Surg HESI Study GuideTravis Hargett93% (14)
- Med Surg CardsDocumento54 pagineMed Surg CardsIanne Merh100% (3)
- Iggy Med Surg Test Bank Chapter 007Documento10 pagineIggy Med Surg Test Bank Chapter 007Tracy Bartell100% (5)
- Medsurg and Pharm HESI ReviewDocumento8 pagineMedsurg and Pharm HESI ReviewSarah Vance100% (4)
- GoodDocumento21 pagineGoodVanessaMUeller80% (5)
- Medsurg ATIDocumento7 pagineMedsurg ATIloveoverpride12% (17)
- Select All That Apply SATADocumento58 pagineSelect All That Apply SATANicholas TagleNessuna valutazione finora
- Blue Print Final Class Med Surg IIDocumento9 pagineBlue Print Final Class Med Surg IIbaconhater100% (1)
- Hurst BurnsDocumento4 pagineHurst BurnsKristin Jones100% (5)
- Med Surg Chapter QuestionsDocumento17 pagineMed Surg Chapter Questionslani75% (4)
- MedSurg3 Test ReviewDocumento30 pagineMedSurg3 Test ReviewAntonella Vitale100% (3)
- Med SurgTest2Documento17 pagineMed SurgTest2Becca Sanborn100% (2)
- Nursing Nclex ExamDocumento11 pagineNursing Nclex ExamDenisa Viviana MaroNessuna valutazione finora
- HESI Test - Free Most Up To Date SampleDocumento13 pagineHESI Test - Free Most Up To Date Sample22oct201481% (32)
- NCLEX Exam Cardiovascular Surgery CareDocumento5 pagineNCLEX Exam Cardiovascular Surgery CareHeather ClemonsNessuna valutazione finora
- Med Surge 2 Mod 3 Study GuideDocumento19 pagineMed Surge 2 Mod 3 Study GuideDirk Buckner100% (4)
- MH AtiDocumento2 pagineMH Atitotodile2395% (19)
- Nclex TipsDocumento23 pagineNclex TipsYA HO100% (2)
- Peds ATI TakeawaysDocumento4 paginePeds ATI TakeawaysNiki95% (19)
- NCLEXDocumento3 pagineNCLEXKath Cuevas50% (2)
- Med-Surg LEWIS 47 Final Foofed UpDocumento10 pagineMed-Surg LEWIS 47 Final Foofed Uphariniliaankhen100% (1)
- Hesi GemsDocumento27 pagineHesi Gemssugarplum22Nessuna valutazione finora
- Medsurg AtiDocumento19 pagineMedsurg AtiShae Thomas88% (17)
- EndocrineDocumento18 pagineEndocrineKristaMaeC.Lazo100% (1)
- NCLEXDocumento10 pagineNCLEXApril Kirstin ChuaNessuna valutazione finora
- Testing - 2 NclexDocumento12 pagineTesting - 2 NclexYoke W KhooNessuna valutazione finora
- 440 - Med Surg HESI 2Documento8 pagine440 - Med Surg HESI 2Chalcey Polson87% (15)
- ATI PN Maternal Newborn NotesDocumento13 pagineATI PN Maternal Newborn NotesDiamond Blackwell100% (6)
- 2019 Rationales HESI TEST BANK MED SURG Version 2Documento1 pagina2019 Rationales HESI TEST BANK MED SURG Version 2Prettygirl71650% (4)
- Nclex-Rn Test Study GuideDocumento199 pagineNclex-Rn Test Study GuideSusan BensonNessuna valutazione finora
- Ignatavicius Renal QuestionsDocumento9 pagineIgnatavicius Renal Questionsboogie02100% (5)
- Chapter 35 - Ignatavicius Medical Surgical NursingDocumento6 pagineChapter 35 - Ignatavicius Medical Surgical Nursinggrkpanygiri100% (4)
- Med-Surg Nusing BulletsDocumento65 pagineMed-Surg Nusing BulletsHarley C. Tan100% (1)
- Cardiovascular Summary Saunders Comprehensive Review For The Nclex RN ExaminationDocumento40 pagineCardiovascular Summary Saunders Comprehensive Review For The Nclex RN ExaminationdanicaNessuna valutazione finora
- Select All That Apply SATADocumento67 pagineSelect All That Apply SATAHermie Joy Maglaqui100% (1)
- Capstone ATI EXIT EXAMDocumento10 pagineCapstone ATI EXIT EXAMcarol50% (2)
- Ignatavicius Chapter 59 (Evolve), Ignatavicius Chapter 57 (Evolve), GI CH 56, 57, 58, 59 Ignatavicius, Ignatavicius Chapter 54 (Evolve), Sole Ch 19, Ignatavicius Chapter 63 (Evolve), Sole Ch 16 Flashcards _ QuizletDocumento63 pagineIgnatavicius Chapter 59 (Evolve), Ignatavicius Chapter 57 (Evolve), GI CH 56, 57, 58, 59 Ignatavicius, Ignatavicius Chapter 54 (Evolve), Sole Ch 19, Ignatavicius Chapter 63 (Evolve), Sole Ch 16 Flashcards _ QuizletNursyNurseNessuna valutazione finora
- NCLEX Study MaterialDocumento40 pagineNCLEX Study MaterialChristie GerconNessuna valutazione finora
- ATI Predictor 2010 Topics To ReviewDocumento8 pagineATI Predictor 2010 Topics To ReviewJonathon95% (19)
- NCLEX (Valerie) PDFDocumento18 pagineNCLEX (Valerie) PDFValerie Orengo100% (1)
- My Nclex Study GuideDocumento4 pagineMy Nclex Study GuideLogin Nurse100% (1)
- NEUROLOGICALDocumento3 pagineNEUROLOGICALRizMarie100% (4)
- Tubes NclexDocumento3 pagineTubes NclexYoke W Khoo100% (1)
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideDa EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNessuna valutazione finora
- Manual VentilationDocumento9 pagineManual VentilationnicoleNessuna valutazione finora
- Why Measure Blood Gases A Threepart Introduction For The Novice Part 3Documento9 pagineWhy Measure Blood Gases A Threepart Introduction For The Novice Part 3Tibi TibiNessuna valutazione finora
- Case Write UpDocumento9 pagineCase Write UpAbdulaziz Al-eisa33% (3)
- PB2 NP3Documento8 paginePB2 NP3Herne BalberdeNessuna valutazione finora
- Modes of Mechanical VentilationDocumento4 pagineModes of Mechanical VentilationDuy ThanhNessuna valutazione finora
- Oxygen Therapy Powerpoint - Jan 2016 Student ViewDocumento47 pagineOxygen Therapy Powerpoint - Jan 2016 Student ViewMark Anthony AlcantaraNessuna valutazione finora
- Daftar PustakaDocumento6 pagineDaftar PustakaCGKN BanyuwangiNessuna valutazione finora
- 2324 Level M (Gr11 UAE - GULF) Biology Practical Booklet-Ch1-6Documento32 pagine2324 Level M (Gr11 UAE - GULF) Biology Practical Booklet-Ch1-6Van halenNessuna valutazione finora
- MsdsDocumento6 pagineMsdsLukman Nul HakimNessuna valutazione finora
- SESIÓN 05 - Parte 2 - TóraxDocumento58 pagineSESIÓN 05 - Parte 2 - TóraxFernando Miguel Calderon CabreraNessuna valutazione finora
- Anatomi HidungDocumento28 pagineAnatomi HidungferyantoachmadNessuna valutazione finora
- Birth AsphyxiaDocumento3 pagineBirth AsphyxiaDebjani MukherjeeNessuna valutazione finora
- Chapter-13 Bio PDFDocumento28 pagineChapter-13 Bio PDFSameer AliNessuna valutazione finora
- Critical CareDocumento25 pagineCritical Carejassen karylle IbanezNessuna valutazione finora
- Adult EDACP Patient Discharge Instructions - March20Documento3 pagineAdult EDACP Patient Discharge Instructions - March20Takisha McpheeNessuna valutazione finora
- Emergency Department Management of Acute Asthma ExacerbationsDocumento32 pagineEmergency Department Management of Acute Asthma ExacerbationsFercho MedNessuna valutazione finora
- 2 NdchestpathDocumento72 pagine2 NdchestpathJhoe Anna Mharie TangoNessuna valutazione finora
- Online CT-1 (Respiration in Humans)Documento5 pagineOnline CT-1 (Respiration in Humans)Sayma AkterNessuna valutazione finora
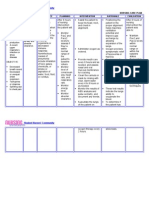
- NCP PneumoniaDocumento2 pagineNCP PneumoniaChristian Apelo Serquillos100% (2)
- Substances Harmful To The Respiratory SystemDocumento25 pagineSubstances Harmful To The Respiratory SystemKar Wai67% (3)
- Material Safety Data Sheet: Section 1. Identification of The Material and SupplierDocumento5 pagineMaterial Safety Data Sheet: Section 1. Identification of The Material and SupplierDAvid Alvarez CastilloNessuna valutazione finora
- Newborn Assessment: By: Ledelle M. de Chavez, Claudine M. Francisco & Don Jayric V. DepalobosDocumento5 pagineNewborn Assessment: By: Ledelle M. de Chavez, Claudine M. Francisco & Don Jayric V. Depalobosdonskii04Nessuna valutazione finora
- ARDSDocumento26 pagineARDSDuratul FahliaNessuna valutazione finora
- Monitoring and Troubleshooting in Mechanical VentilatorDocumento77 pagineMonitoring and Troubleshooting in Mechanical VentilatorRashma Little RobinNessuna valutazione finora
- Critical Care Therapy and Respiratory Care Section: 1.0 DescriptionDocumento7 pagineCritical Care Therapy and Respiratory Care Section: 1.0 DescriptionLenny Ronalyn QuitorianoNessuna valutazione finora
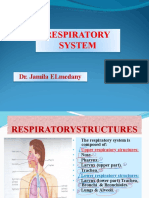
- Respiratory SystemhjhuDocumento23 pagineRespiratory SystemhjhuSara ANessuna valutazione finora
- Conceptual Study of Pranavaha Strotas With Reference To Modern AnatomyDocumento6 pagineConceptual Study of Pranavaha Strotas With Reference To Modern AnatomyRahimshaikhNessuna valutazione finora
- UWorld NCLEX-RN QBank 2018 PDFDocumento103 pagineUWorld NCLEX-RN QBank 2018 PDFIlluminatis99% (90)
- Imaging of Pneumothorax - UpToDateDocumento40 pagineImaging of Pneumothorax - UpToDateTP RMadNessuna valutazione finora