Potrebbero piacerti anche
- ECG Rhythm InterpretationDocumento208 pagineECG Rhythm InterpretationMariah WaelNessuna valutazione finora
- ECGDocumento154 pagineECGSandeep BansalNessuna valutazione finora
- ECG Rhythm Interpretation: Recognize Arrhythmias and Interpret ECGsDocumento232 pagineECG Rhythm Interpretation: Recognize Arrhythmias and Interpret ECGslaureeateNessuna valutazione finora
- ECG Rhythm InterpretationDocumento200 pagineECG Rhythm InterpretationabramNessuna valutazione finora
- ECG InterpretationDocumento108 pagineECG InterpretationMohammad SalehNessuna valutazione finora
- ECG UpdatedDocumento115 pagineECG Updatedmominarasool7Nessuna valutazione finora
- EkgDocumento21 pagineEkgElsye FitriasariNessuna valutazione finora
- Normal Impulse Conduction: Sinoatrial NodeDocumento80 pagineNormal Impulse Conduction: Sinoatrial Nodesiusiuwidyanto100% (2)
- EKG DasarDocumento54 pagineEKG Dasarseptiyana indahpraptiwiNessuna valutazione finora
- ECG Rhythm Interpretation: Sinus Rhythms and Premature BeatsDocumento22 pagineECG Rhythm Interpretation: Sinus Rhythms and Premature BeatsSamer ThaherNessuna valutazione finora
- ECG Module 4aDocumento22 pagineECG Module 4aDexter GabrielNessuna valutazione finora
- Module 4a.heart ArryhtmiasDocumento22 pagineModule 4a.heart ArryhtmiasFerry SofyanriNessuna valutazione finora
- Cara Membaca EKG Lengkap PAluDocumento214 pagineCara Membaca EKG Lengkap PAluGiriNessuna valutazione finora
- ECG Rhythm Interpretation: Module IV ADocumento21 pagineECG Rhythm Interpretation: Module IV AImim NozNessuna valutazione finora
- IVA. Heart ArrhythmiasDocumento21 pagineIVA. Heart ArrhythmiasJohn Christopher P. TiamzonNessuna valutazione finora
- Module - 1 EkgDocumento11 pagineModule - 1 EkgCarmen CiursaşNessuna valutazione finora
- ECG Rhythm Interpretation GuideDocumento11 pagineECG Rhythm Interpretation GuideFerry SofyanriNessuna valutazione finora
- Module 4bDocumento22 pagineModule 4bSamer ThaherNessuna valutazione finora
- Cardiac Arrest: April B. Perez, RN, Man, PHD, FpchaDocumento50 pagineCardiac Arrest: April B. Perez, RN, Man, PHD, Fpchayuuki konnoNessuna valutazione finora
- ECG Interpretations DR RPDocumento109 pagineECG Interpretations DR RPArnis Putri RosyaniNessuna valutazione finora
- ECG Learning ModulesDocumento150 pagineECG Learning ModulesdodiNessuna valutazione finora
- WWW - Medicalppt.: For More Free Medical Powerpoint Presentations Visit WebsiteDocumento24 pagineWWW - Medicalppt.: For More Free Medical Powerpoint Presentations Visit WebsitezaheerbdsNessuna valutazione finora
- EkgDocumento67 pagineEkgFendi Rafif Dad'sNessuna valutazione finora
- WWW - Medicalppt.: For More Free Medical Powerpoint Presentations Visit WebsiteDocumento24 pagineWWW - Medicalppt.: For More Free Medical Powerpoint Presentations Visit WebsiteSergiu HelciugNessuna valutazione finora
- Learning ECGDocumento187 pagineLearning ECGPhysiology by Dr Raghuveer100% (2)
- WWW - Medicalppt.: For More Free Medical Powerpoint Presentations Visit WebsiteDocumento16 pagineWWW - Medicalppt.: For More Free Medical Powerpoint Presentations Visit WebsiteSujith RaoNessuna valutazione finora
- Pemasangan Dan Interpretasi EKGDocumento117 paginePemasangan Dan Interpretasi EKGaulianadanisya100% (2)
- Basics of ECGDocumento32 pagineBasics of ECGNachiket Vijay PotdarNessuna valutazione finora
- ECG Module 3Documento14 pagineECG Module 3ibnbasheer100% (3)
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocumento74 pagineBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- Gamal Abd EL Nasser Mahmoud: Prepared ByDocumento64 pagineGamal Abd EL Nasser Mahmoud: Prepared ByMohamed ElkadyNessuna valutazione finora
- Basic Ecg InterpretationDocumento88 pagineBasic Ecg Interpretationtristan keeNessuna valutazione finora
- Nursing School EKGDocumento43 pagineNursing School EKGRob Dickerson100% (1)
- Approach To ACLS RhythmDocumento150 pagineApproach To ACLS RhythmChristine Bernadette Rapal Bollong100% (2)
- ECG MonitoringDocumento96 pagineECG MonitoringJey BautistaNessuna valutazione finora
- Module 4aDocumento24 pagineModule 4aMaseaNessuna valutazione finora
- ECG Rhythm Interpretation: Module IV CDocumento18 pagineECG Rhythm Interpretation: Module IV CFauzi RahmanNessuna valutazione finora
- PacemakerDocumento156 paginePacemakerDhruv DesaiNessuna valutazione finora
- Sinus Brad, Tach, PAC, PVCDocumento17 pagineSinus Brad, Tach, PAC, PVCEdRobertArnadNessuna valutazione finora
- ECG Basics Lecture 1Documento116 pagineECG Basics Lecture 1AreebaNessuna valutazione finora
- Kuliah EKG Blok Kegawatdaruratan September 2018Documento122 pagineKuliah EKG Blok Kegawatdaruratan September 2018khanzaisdiharanaNessuna valutazione finora
- Ecg Interpretation New TemplateDocumento88 pagineEcg Interpretation New TemplateJonathan NgNessuna valutazione finora
- Prof. Maila Claire A. Lichauco, RN, MANDocumento86 pagineProf. Maila Claire A. Lichauco, RN, MANCedie GomezNessuna valutazione finora
- ELECTROCARDIOGRAMDocumento63 pagineELECTROCARDIOGRAMMbah GapinbissiNessuna valutazione finora
- EKG Interpretasi Dan Lethal Aritmia: Aan NuraeniDocumento34 pagineEKG Interpretasi Dan Lethal Aritmia: Aan NuraeniCitra Marchelina Novilini100% (1)
- Pontianak Baca Ekg Des 2014Documento175 paginePontianak Baca Ekg Des 2014Nur Rahmat WibowoNessuna valutazione finora
- Module 4bDocumento24 pagineModule 4bMaseaNessuna valutazione finora
- N12 Cardiac DysrhythmiasDocumento68 pagineN12 Cardiac Dysrhythmiaskathbondoc03Nessuna valutazione finora
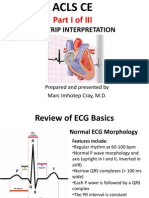
- ACLS CE-Part I of III - ECG Strip Interpretation W Case Scenarios SupplementalDocumento80 pagineACLS CE-Part I of III - ECG Strip Interpretation W Case Scenarios SupplementalMarc Imhotep Cray, M.D.100% (2)
- ECG InterpretationDocumento52 pagineECG InterpretationMarcus, RN98% (44)
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookDa EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNessuna valutazione finora
- Guide to Canine and Feline ElectrocardiographyDa EverandGuide to Canine and Feline ElectrocardiographyRuth WillisNessuna valutazione finora
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasDa EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasValutazione: 3 su 5 stelle3/5 (5)
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisDa EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisValutazione: 5 su 5 stelle5/5 (1)
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Da EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Nessuna valutazione finora
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsDa EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNessuna valutazione finora
- Heamophilia ResearchDocumento21 pagineHeamophilia ResearchRohini SelvarajahNessuna valutazione finora
- Doctor's skills and experienceDocumento5 pagineDoctor's skills and experienceRohini Selvarajah67% (3)
- ScabiesDocumento14 pagineScabiesRohini SelvarajahNessuna valutazione finora
- Antidepressant Medication: Advice For AdultsDocumento4 pagineAntidepressant Medication: Advice For AdultsRohini SelvarajahNessuna valutazione finora
- Basal Cell Carcinoma Squamous Cell Carcinoma Guide Nov 2008-Final With CorrigendumsDocumento183 pagineBasal Cell Carcinoma Squamous Cell Carcinoma Guide Nov 2008-Final With CorrigendumsBoofy27Nessuna valutazione finora
- Mental State ExaminationDocumento5 pagineMental State ExaminationRohini SelvarajahNessuna valutazione finora
- CP 111Documento246 pagineCP 111Yhr YhNessuna valutazione finora
- WWW - Medicalppt.: For More Free Medical Powerpoint Presentations Visit WebsiteDocumento27 pagineWWW - Medicalppt.: For More Free Medical Powerpoint Presentations Visit Websitevanstar7Nessuna valutazione finora
- Free Medical ECG Interpretation PresentationsDocumento30 pagineFree Medical ECG Interpretation PresentationsRohini SelvarajahNessuna valutazione finora
- Melanoma and Other Skin CancersDocumento4 pagineMelanoma and Other Skin CancersRohini SelvarajahNessuna valutazione finora
- Topical Issues in DermatologyDocumento8 pagineTopical Issues in DermatologyRohini SelvarajahNessuna valutazione finora
- ScabiesDocumento14 pagineScabiesRohini SelvarajahNessuna valutazione finora
- Disorders of thought form and memory disordersDocumento41 pagineDisorders of thought form and memory disordersRohini SelvarajahNessuna valutazione finora
- Handout For Using Antipsychotic TherapyDocumento4 pagineHandout For Using Antipsychotic TherapyRohini SelvarajahNessuna valutazione finora
- Depression in Pregnancy & Antidepressant Medication UseDocumento2 pagineDepression in Pregnancy & Antidepressant Medication UseRohini SelvarajahNessuna valutazione finora
- Intimate Partner ViolenceDocumento5 pagineIntimate Partner ViolenceRohini SelvarajahNessuna valutazione finora
- Antibiotics Is Soft Tissue InfectionDocumento6 pagineAntibiotics Is Soft Tissue InfectionRohini SelvarajahNessuna valutazione finora
- Sleep DisordersDocumento32 pagineSleep DisordersRohini Selvarajah100% (1)
- Alcohol Intervention - What WorksDocumento4 pagineAlcohol Intervention - What WorksRohini SelvarajahNessuna valutazione finora
- Alcohol Misuse and DependenceDocumento7 pagineAlcohol Misuse and DependenceRohini SelvarajahNessuna valutazione finora
- Tarik Recalls 9-11-2012Documento28 pagineTarik Recalls 9-11-2012Rohini SelvarajahNessuna valutazione finora
- Vaccination During PregnancyDocumento13 pagineVaccination During PregnancyRohini SelvarajahNessuna valutazione finora
- ++mariam - S Recalls Feb. 2014444Documento15 pagine++mariam - S Recalls Feb. 2014444Rohini SelvarajahNessuna valutazione finora
- Cairan IntravenaDocumento187 pagineCairan IntravenaRizky DimasaputraNessuna valutazione finora
- 15 March 2014Documento14 pagine15 March 2014Rohini Selvarajah100% (2)
- WWW - Medicalppt.: For More Free Medical Powerpoint Presentations Visit WebsiteDocumento27 pagineWWW - Medicalppt.: For More Free Medical Powerpoint Presentations Visit Websitevanstar7Nessuna valutazione finora
- Tehreem - Recalls MODIFIED BY Me & AARAVDocumento58 pagineTehreem - Recalls MODIFIED BY Me & AARAVRohini SelvarajahNessuna valutazione finora
- 15 Feb 2014.doc HinaDocumento12 pagine15 Feb 2014.doc HinaRohini SelvarajahNessuna valutazione finora
- Drug KardexDocumento1 paginaDrug KardexRohini SelvarajahNessuna valutazione finora
- Application For AmendingDocumento4 pagineApplication For AmendingRohini SelvarajahNessuna valutazione finora
- KoyoDocumento4 pagineKoyovichitNessuna valutazione finora
- Concept Page - Using Vagrant On Your Personal Computer - Holberton Intranet PDFDocumento7 pagineConcept Page - Using Vagrant On Your Personal Computer - Holberton Intranet PDFJeffery James DoeNessuna valutazione finora
- Answer Key p2 p1Documento95 pagineAnswer Key p2 p1Nafisa AliNessuna valutazione finora
- Quaternary Protoberberine Alkaloids (Must Read)Documento26 pagineQuaternary Protoberberine Alkaloids (Must Read)Akshay AgnihotriNessuna valutazione finora
- Air Wellness QRSDocumento2 pagineAir Wellness QRSapi-3743459Nessuna valutazione finora
- The Impact of Employees' Commitment Towards Food Safety at Ayana Resort, BaliDocumento58 pagineThe Impact of Employees' Commitment Towards Food Safety at Ayana Resort, Balirachelle agathaNessuna valutazione finora
- Who will buy electric vehicles Segmenting the young Indian buyers using cluster analysisDocumento12 pagineWho will buy electric vehicles Segmenting the young Indian buyers using cluster analysisbhasker sharmaNessuna valutazione finora
- DENSO COMMON RAIL INJECTOR REPAIR GUIDEDocumento22 pagineDENSO COMMON RAIL INJECTOR REPAIR GUIDEMarcoNessuna valutazione finora
- Telco XPOL MIMO Industrial Class Solid Dish AntennaDocumento4 pagineTelco XPOL MIMO Industrial Class Solid Dish AntennaOmar PerezNessuna valutazione finora
- GIS AccidentsDocumento5 pagineGIS Accidentsali110011Nessuna valutazione finora
- Caterpillar Ep15krtDocumento37 pagineCaterpillar Ep15krtIvan MajikNessuna valutazione finora
- Features Integration of Differential Binomial: DX BX A X P N MDocumento4 pagineFeatures Integration of Differential Binomial: DX BX A X P N Mابو سامرNessuna valutazione finora
- Product ListDocumento4 pagineProduct ListyuvashreeNessuna valutazione finora
- Entrepreneurship Project On Jam, Jelly & PicklesDocumento24 pagineEntrepreneurship Project On Jam, Jelly & Picklesashish karshinkarNessuna valutazione finora
- Placenta Previa Case Study: Adefuin, Jay Rovillos, Noemie MDocumento40 paginePlacenta Previa Case Study: Adefuin, Jay Rovillos, Noemie MMikes CastroNessuna valutazione finora
- De Thi HSG Tinh Binh PhuocDocumento9 pagineDe Thi HSG Tinh Binh PhuocDat Do TienNessuna valutazione finora
- Effect of Some Algal Filtrates and Chemical Inducers On Root-Rot Incidence of Faba BeanDocumento7 pagineEffect of Some Algal Filtrates and Chemical Inducers On Root-Rot Incidence of Faba BeanJuniper PublishersNessuna valutazione finora
- Uhf Leaky Feeder Rev CDocumento4 pagineUhf Leaky Feeder Rev CLuis Isaac PadillaNessuna valutazione finora
- Monster of The Week Tome of Mysteries PlaybooksDocumento10 pagineMonster of The Week Tome of Mysteries PlaybooksHyperLanceite XNessuna valutazione finora
- Ancient MesopotamiaDocumento69 pagineAncient MesopotamiaAlma CayapNessuna valutazione finora
- 7890 Parts-Guide APDocumento4 pagine7890 Parts-Guide APZia HaqNessuna valutazione finora
- Flood FillDocumento1 paginaFlood FillshubhamNessuna valutazione finora
- Evolutionary PsychologyDocumento10 pagineEvolutionary PsychologyShreya MadheswaranNessuna valutazione finora
- QP (2016) 2Documento1 paginaQP (2016) 2pedro carrapicoNessuna valutazione finora
- Religion in Space Science FictionDocumento23 pagineReligion in Space Science FictionjasonbattNessuna valutazione finora
- The Simple PendulumDocumento5 pagineThe Simple PendulumDexter TorringtonNessuna valutazione finora
- Smart Note Taker Saves Time With Air WritingDocumento17 pagineSmart Note Taker Saves Time With Air WritingNagarjuna LokkuNessuna valutazione finora
- Cs8791 Cloud Computing Unit2 NotesDocumento37 pagineCs8791 Cloud Computing Unit2 NotesTeju MelapattuNessuna valutazione finora
- Taking Back SundayDocumento9 pagineTaking Back SundayBlack CrowNessuna valutazione finora