Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Avatar Legends The Roleplaying Game 1 12Documento12 pagineAvatar Legends The Roleplaying Game 1 12azeaze0% (1)
- (Michael Farber) Invitation To Topological RoboticDocumento145 pagine(Michael Farber) Invitation To Topological RoboticLeonora C. Ford100% (3)
- Case Study Alliston AssignmentDocumento6 pagineCase Study Alliston AssignmentParamvir SinghNessuna valutazione finora
- Ati Codes Cont'Documento1 paginaAti Codes Cont'm1k0eNessuna valutazione finora
- Hesi Entrance Examination Study GuideDocumento195 pagineHesi Entrance Examination Study Guidetken35100% (2)
- Vlue AdDocumento153 pagineVlue AdsindhushankarNessuna valutazione finora
- Invoice Ce 2019 12 IVDocumento8 pagineInvoice Ce 2019 12 IVMoussa NdourNessuna valutazione finora
- First Quarter-Module 2-Lesson 2-21st Century Literature From The Philippines and The WorldDocumento25 pagineFirst Quarter-Module 2-Lesson 2-21st Century Literature From The Philippines and The WorldAndrea Ibañez73% (11)
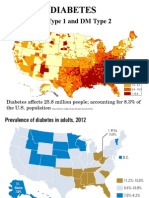
- Endo DM Type 1 and 2Documento35 pagineEndo DM Type 1 and 2m1k0eNessuna valutazione finora
- ATI CollaborationDocumento46 pagineATI Collaborationm1k0e72% (29)
- LicenseDocumento7 pagineLicenseAdnan AvdukićNessuna valutazione finora
- Monthly Membership Subscription FAQsDocumento2 pagineMonthly Membership Subscription FAQsm1k0eNessuna valutazione finora
- How Bankruptcy Affects Real Estate Titles and Bankruptcy Risks Covered by Title Insurance - 00104887Documento11 pagineHow Bankruptcy Affects Real Estate Titles and Bankruptcy Risks Covered by Title Insurance - 00104887m1k0eNessuna valutazione finora
- Hyponatremia: Symptoms May Vary With Changes in Vascular VolumeDocumento3 pagineHyponatremia: Symptoms May Vary With Changes in Vascular Volumem1k0eNessuna valutazione finora
- ATIpendixDocumento38 pagineATIpendixm1k0e100% (1)
- Reconstitution & IVPB Delivery of Medication Check ofDocumento3 pagineReconstitution & IVPB Delivery of Medication Check ofm1k0eNessuna valutazione finora
- Osteoarthritis, Hip Replacement, OsteoporosisDocumento19 pagineOsteoarthritis, Hip Replacement, Osteoporosism1k0eNessuna valutazione finora
- HTN - Sodium PPT EditionDocumento15 pagineHTN - Sodium PPT Editionm1k0eNessuna valutazione finora
- Mus Culo Skeletal Exam OutlineDocumento14 pagineMus Culo Skeletal Exam Outlinem1k0eNessuna valutazione finora
- Introduction To Pediatric Nursing 2012 Student VersionDocumento71 pagineIntroduction To Pediatric Nursing 2012 Student Versionm1k0eNessuna valutazione finora
- Antimicrobial Stewardship: Attempting To Preserve A Strategic ResourceDocumento7 pagineAntimicrobial Stewardship: Attempting To Preserve A Strategic Resourcem1k0eNessuna valutazione finora
- The Pattern of Antimicrobial Use For Palliative Care In-Patients During The Last Week of LifeDocumento4 pagineThe Pattern of Antimicrobial Use For Palliative Care In-Patients During The Last Week of Lifem1k0eNessuna valutazione finora
- HTN - Sodium PPT EditionDocumento15 pagineHTN - Sodium PPT Editionm1k0eNessuna valutazione finora
- MGMT E-2000 Fall 2014 SyllabusDocumento13 pagineMGMT E-2000 Fall 2014 Syllabusm1k0eNessuna valutazione finora
- Medicine American Journal of Hospice and PalliativeDocumento6 pagineMedicine American Journal of Hospice and Palliativem1k0eNessuna valutazione finora
- Reducing Inappropriate Antibiotic Prescribing in The Residential Care Setting: Current PerspectivesDocumento13 pagineReducing Inappropriate Antibiotic Prescribing in The Residential Care Setting: Current Perspectivesm1k0eNessuna valutazione finora
- Health & Physical Assessment in Nursing: Donita D'Amico Colleen BarbaritoDocumento48 pagineHealth & Physical Assessment in Nursing: Donita D'Amico Colleen Barbaritom1k0eNessuna valutazione finora
- EKG Crash Course NuRsing 390 SMC - 4Documento57 pagineEKG Crash Course NuRsing 390 SMC - 4m1k0e100% (2)
- Effectiveness of A Comprehensive Hand Hygiene Program ForDocumento11 pagineEffectiveness of A Comprehensive Hand Hygiene Program Form1k0eNessuna valutazione finora
- Effectiveness of A Comprehensive Hand Hygiene Program ForDocumento11 pagineEffectiveness of A Comprehensive Hand Hygiene Program Form1k0eNessuna valutazione finora
- Obtaining A Pap SmearDocumento1 paginaObtaining A Pap Smearm1k0eNessuna valutazione finora
- Atoal Material Safety Data SheetsDocumento1 paginaAtoal Material Safety Data Sheetsm1k0eNessuna valutazione finora
- 7211 Vitamin K 2014Documento42 pagine7211 Vitamin K 2014m1k0eNessuna valutazione finora
- Guide To UspsDocumento28 pagineGuide To Uspsm1k0eNessuna valutazione finora
- Chapter 3 Macromolecules and The Origin of LifeDocumento13 pagineChapter 3 Macromolecules and The Origin of Lifem1k0eNessuna valutazione finora
- Chapter 003Documento2 pagineChapter 003m1k0eNessuna valutazione finora
- PPH CasestudyDocumento45 paginePPH CasestudyRona Mae PangilinanNessuna valutazione finora
- Of Bones and Buddhas Contemplation of TH PDFDocumento215 pagineOf Bones and Buddhas Contemplation of TH PDFCNessuna valutazione finora
- 7A Detailed Lesson Plan in Health 7 I. Content Standard: Teacher's Activity Students' ActivityDocumento10 pagine7A Detailed Lesson Plan in Health 7 I. Content Standard: Teacher's Activity Students' ActivityLeizel C. LeonidoNessuna valutazione finora
- VTU Result PDFDocumento2 pagineVTU Result PDFVaibhavNessuna valutazione finora
- Teaching Philosophy StatementDocumento25 pagineTeaching Philosophy Statementtchrdale27Nessuna valutazione finora
- 3.1 Learning To Be A Better StudentDocumento27 pagine3.1 Learning To Be A Better StudentApufwplggl JomlbjhfNessuna valutazione finora
- Basic Trigonometric FunctionDocumento34 pagineBasic Trigonometric FunctionLony PatalNessuna valutazione finora
- Virtue EpistemologyDocumento32 pagineVirtue EpistemologyJorge Torres50% (2)
- Fsi GreekBasicCourse Volume1 StudentTextDocumento344 pagineFsi GreekBasicCourse Volume1 StudentTextbudapest1Nessuna valutazione finora
- Procedures: Step 1 Freeze or Restrain The Suspect/sDocumento5 pagineProcedures: Step 1 Freeze or Restrain The Suspect/sRgenieDictadoNessuna valutazione finora
- Journal of Cleaner Production: Kamalakanta Muduli, Kannan Govindan, Akhilesh Barve, Yong GengDocumento10 pagineJournal of Cleaner Production: Kamalakanta Muduli, Kannan Govindan, Akhilesh Barve, Yong GengAnass CHERRAFINessuna valutazione finora
- Si493b 1Documento3 pagineSi493b 1Sunil KhadkaNessuna valutazione finora
- Boxnhl MBS (Design-D) Check SheetDocumento13 pagineBoxnhl MBS (Design-D) Check SheetKumari SanayaNessuna valutazione finora
- DBI Setup Steps For Procurement IntelligenceDocumento4 pagineDBI Setup Steps For Procurement IntelligenceAnubhav.MittalNessuna valutazione finora
- Axis Bank - Hoam LoanDocumento21 pagineAxis Bank - Hoam LoansonamNessuna valutazione finora
- The Endless Pursuit of Truth: Subalternity and Marginalization in Post-Neorealist Italian FilmDocumento206 pagineThe Endless Pursuit of Truth: Subalternity and Marginalization in Post-Neorealist Italian FilmPaul MathewNessuna valutazione finora
- Decision Making and Problem Solving & Managing - Gashaw PDFDocumento69 pagineDecision Making and Problem Solving & Managing - Gashaw PDFKokebu MekonnenNessuna valutazione finora
- δ (n) = u (n) - u (n-3) = 1 ,n=0Documento37 pagineδ (n) = u (n) - u (n-3) = 1 ,n=0roberttheivadasNessuna valutazione finora
- Evaluation of The Performance of HRCT in The Diagnostic and Management of Covid-19Documento7 pagineEvaluation of The Performance of HRCT in The Diagnostic and Management of Covid-19IJAR JOURNALNessuna valutazione finora
- Dollar Unit SamplingDocumento7 pagineDollar Unit SamplingAndriatsirihasinaNessuna valutazione finora
- Chemistry Chapter SummariesDocumento23 pagineChemistry Chapter SummariesHayley AndersonNessuna valutazione finora
- Pitch PDFDocumento12 paginePitch PDFJessa Mae AnonuevoNessuna valutazione finora
- Azadegan VadoodDocumento100 pagineAzadegan VadoodadeeyoNessuna valutazione finora
- Your ManDocumento5 pagineYour ManPaulino JoaquimNessuna valutazione finora