Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Holidays Homework 12Documento26 pagineHolidays Homework 12richa agarwalNessuna valutazione finora
- Class 11 Biology Notes Chapter 2 Studyguide360Documento10 pagineClass 11 Biology Notes Chapter 2 Studyguide360ANessuna valutazione finora
- Introduction To Personal FinanceDocumento15 pagineIntroduction To Personal FinanceMa'am Katrina Marie MirandaNessuna valutazione finora
- Percussion Catalog Eu Lep2001Documento24 paginePercussion Catalog Eu Lep2001isaac HernandezNessuna valutazione finora
- ArcSight Profiler IntegrationDocumento8 pagineArcSight Profiler IntegrationemveNessuna valutazione finora
- 1404 1284 PDFDocumento150 pagine1404 1284 PDFJohannRoaNessuna valutazione finora
- KNOLL and HIERY, The German Colonial Experience - IntroDocumento6 pagineKNOLL and HIERY, The German Colonial Experience - IntroGloria MUNessuna valutazione finora
- Introduction To Mechanical Engineering Si Edition 4Th Edition Wickert Lewis 1305635752 9781305635753 Solution Manual Full Chapter PDFDocumento36 pagineIntroduction To Mechanical Engineering Si Edition 4Th Edition Wickert Lewis 1305635752 9781305635753 Solution Manual Full Chapter PDFwilliam.munoz276100% (13)
- Battle RoyaleDocumento4 pagineBattle RoyalerwNessuna valutazione finora
- Banana Oil LabDocumento5 pagineBanana Oil LabjbernayNessuna valutazione finora
- Rule 108 Republic Vs TipayDocumento1 paginaRule 108 Republic Vs TipayShimi Fortuna100% (1)
- 1 Hot Metal Tapping SOPDocumento25 pagine1 Hot Metal Tapping SOPSANJAY KUMAR PATINessuna valutazione finora
- Sow English Year 4 2023 2024Documento12 pagineSow English Year 4 2023 2024Shamien ShaNessuna valutazione finora
- Internship Report Aqib 2Documento11 pagineInternship Report Aqib 2Usman SheikhNessuna valutazione finora
- Auto Loan Application Form - IndividualDocumento2 pagineAuto Loan Application Form - IndividualKlarise EspinosaNessuna valutazione finora
- FS0008 Toolangi State Forest Walking TrailsDocumento2 pagineFS0008 Toolangi State Forest Walking TrailsMichael ConosNessuna valutazione finora
- BI410 Plant Developmental BiologyDocumento41 pagineBI410 Plant Developmental BiologyLaisla CagliariNessuna valutazione finora
- BY DR Muhammad Akram M.C.H.JeddahDocumento32 pagineBY DR Muhammad Akram M.C.H.JeddahMuhammad Akram Qaim KhaniNessuna valutazione finora
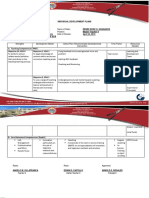
- Individual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Documento2 pagineIndividual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Angelo VillafrancaNessuna valutazione finora
- WLP Math Week 4 Q4Documento4 pagineWLP Math Week 4 Q4JUDELYN O. DOMINGONessuna valutazione finora
- FinTech and Banking DisruptionDocumento13 pagineFinTech and Banking DisruptionMaru MasNessuna valutazione finora
- DRTA-directed Reading Thinking Activity: M. Truscott Staff Development 9-24-10Documento13 pagineDRTA-directed Reading Thinking Activity: M. Truscott Staff Development 9-24-10ehaines24Nessuna valutazione finora
- Jyotsna G. Singh - Shakespeare and Postcolonial Theory (2019)Documento265 pagineJyotsna G. Singh - Shakespeare and Postcolonial Theory (2019)luisaNessuna valutazione finora
- Snowman Card Game PDFDocumento2 pagineSnowman Card Game PDFFOANessuna valutazione finora
- 2202 Infantilization Essay - Quinn WilsonDocumento11 pagine2202 Infantilization Essay - Quinn Wilsonapi-283151250Nessuna valutazione finora
- Gremath Set8-1Documento48 pagineGremath Set8-1uzairmetallurgistNessuna valutazione finora
- 9 - Report & NarrativeDocumento1 pagina9 - Report & NarrativeTri WahyuningsihNessuna valutazione finora
- Amazon PrimeDocumento27 pagineAmazon PrimeMohamedNessuna valutazione finora
- Napoleon Lacroze Von Sanden - Crony Capitalism in ArgentinaDocumento1 paginaNapoleon Lacroze Von Sanden - Crony Capitalism in ArgentinaBoney LacrozeNessuna valutazione finora
- Oblicon NotesDocumento14 pagineOblicon NotesCee Silo Aban100% (1)