Potrebbero piacerti anche
- Congenital Glaucomas: 1. Primary 2. Iridocorneal DysgenesisDocumento12 pagineCongenital Glaucomas: 1. Primary 2. Iridocorneal DysgenesiskhadzxNessuna valutazione finora
- Primary Angle-Closure Glaucoma: 1. Pathogenesis 2. ClassificationDocumento9 paginePrimary Angle-Closure Glaucoma: 1. Pathogenesis 2. ClassificationkhadzxNessuna valutazione finora
- 34 Idiopathic Spec Uveitis SyndromeDocumento8 pagine34 Idiopathic Spec Uveitis SyndromekhadzxNessuna valutazione finora
- 15corneal InfectionsDocumento8 pagine15corneal InfectionskhadzxNessuna valutazione finora
- Congenital Cataract: 1. Important FactsDocumento13 pagineCongenital Cataract: 1. Important FactskhadzxNessuna valutazione finora
- Acquired 2. Isolated Familial Ectopia Lentis 3. Associated With Systemic SyndromesDocumento8 pagineAcquired 2. Isolated Familial Ectopia Lentis 3. Associated With Systemic SyndromeskhadzxNessuna valutazione finora
- Abnormal Lens ShapeDocumento4 pagineAbnormal Lens ShapekhadzxNessuna valutazione finora
- Sudden Unexpected Death FMT 400Documento11 pagineSudden Unexpected Death FMT 400khadzxNessuna valutazione finora
- 02chronic Marginal BlepharitisDocumento7 pagine02chronic Marginal BlepharitiskhadzxNessuna valutazione finora
- Chronic Osteomyelitis in Early Infancy: Presenter: DR Maina Discussant: DR Mogire (Orthopedic Surgeon)Documento27 pagineChronic Osteomyelitis in Early Infancy: Presenter: DR Maina Discussant: DR Mogire (Orthopedic Surgeon)khadzxNessuna valutazione finora
- Juvenile Rheumatoid Arthritis (Jra) (Juvenile Chronic Arthritis-Jca)Documento70 pagineJuvenile Rheumatoid Arthritis (Jra) (Juvenile Chronic Arthritis-Jca)khadzxNessuna valutazione finora
- Disorders of Eye LashesDocumento8 pagineDisorders of Eye LasheskhadzxNessuna valutazione finora
- Ndiang'Ui: Unexpected Deaths 24 September 2009Documento25 pagineNdiang'Ui: Unexpected Deaths 24 September 2009khadzxNessuna valutazione finora
- Postmortem Changes and Postmortem Time IntervalDocumento24 paginePostmortem Changes and Postmortem Time IntervalkhadzxNessuna valutazione finora
- Introduction To Forensic Medicine DR David Chumba MBCHB, Mmed (Human Pathology), Dip. For Med (Sa)Documento20 pagineIntroduction To Forensic Medicine DR David Chumba MBCHB, Mmed (Human Pathology), Dip. For Med (Sa)khadzxNessuna valutazione finora
- Narcotics N HallucinogensDocumento14 pagineNarcotics N HallucinogenskhadzxNessuna valutazione finora
- Fire Arm Injuries 4th Yr ForensicDocumento31 pagineFire Arm Injuries 4th Yr ForensickhadzxNessuna valutazione finora
- Poisoning by MedicinesDocumento11 paginePoisoning by MedicineskhadzxNessuna valutazione finora
- Carbon Monoxide Poisoning 4th YrDocumento17 pagineCarbon Monoxide Poisoning 4th YrkhadzxNessuna valutazione finora
- Classification of Injuries FMTDocumento30 pagineClassification of Injuries FMTkhadzx100% (2)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Get Shredded v2.0Documento30 pagineGet Shredded v2.0Jaldeep RekhiNessuna valutazione finora
- Tissue Salt Primer SchuesslerDocumento36 pagineTissue Salt Primer SchuesslerYanka IlarionovaNessuna valutazione finora
- Nutrition and Dietetics Midterm Exam October 2018Documento14 pagineNutrition and Dietetics Midterm Exam October 2018Daniel Laoaten100% (2)
- Manual of Pediatric NutritionDocumento598 pagineManual of Pediatric NutritionjuniarsihsrkNessuna valutazione finora
- My Project Now 5Documento40 pagineMy Project Now 5Stonedollar20Nessuna valutazione finora
- Conditioning Lesson 1Documento4 pagineConditioning Lesson 1Jake ElliottNessuna valutazione finora
- Owner S Manual: Questions?Documento16 pagineOwner S Manual: Questions?Marc SchwartzNessuna valutazione finora
- COCO Tugi BarsDocumento23 pagineCOCO Tugi BarsJohanz PacrisNessuna valutazione finora
- The Role of Medications in Weight LossDocumento14 pagineThe Role of Medications in Weight LossWareesa JamshedNessuna valutazione finora
- Food Additives Report 2010 FINALDocumento64 pagineFood Additives Report 2010 FINALMinh Nguyen MinhNessuna valutazione finora
- Rindermann, H. 2018. "Causes of National and Historical Differences in Cognitive Ability - and Reciprocal Effects"Documento146 pagineRindermann, H. 2018. "Causes of National and Historical Differences in Cognitive Ability - and Reciprocal Effects"YmeNessuna valutazione finora
- Pineal XTDocumento3 paginePineal XTMr TellerzNessuna valutazione finora
- Case StudyDocumento3 pagineCase StudyXosweetbebeNessuna valutazione finora
- PBL Thematic - 3Documento9 paginePBL Thematic - 3Rakshith KumarNessuna valutazione finora
- Reading Part A AppendicitisDocumento6 pagineReading Part A Appendicitisfernanda1rondelli0% (2)
- Nursing Care Plan - CancerDocumento3 pagineNursing Care Plan - CancerChristineAla0% (1)
- Why Spirulina Boosts Your Energy LevelDocumento1 paginaWhy Spirulina Boosts Your Energy LevelpinaslifeNessuna valutazione finora
- Enteral Nutrition - Yudhi AdriantoDocumento41 pagineEnteral Nutrition - Yudhi AdriantoAri SusandiNessuna valutazione finora
- Meal Mentor Sample Meal PlanDocumento20 pagineMeal Mentor Sample Meal Planverdes nicoletaNessuna valutazione finora
- UNILEVER Green ManufacturingDocumento20 pagineUNILEVER Green ManufacturingLavina MehtaNessuna valutazione finora
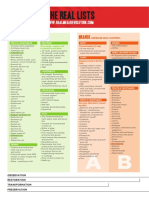
- Real Meal RevolutionTHE-LIST-A4Documento2 pagineReal Meal RevolutionTHE-LIST-A4fridayschild2012Nessuna valutazione finora
- 2390-Article Text-4383 ChokoDocumento5 pagine2390-Article Text-4383 ChokoanaaaNessuna valutazione finora
- GHK, Probiotics - Sept 12Documento3 pagineGHK, Probiotics - Sept 12Shyden Taghap Billones BordaNessuna valutazione finora
- Business PlanDocumento4 pagineBusiness Plannainaa18Nessuna valutazione finora
- Ncp1 317rle Ronquillo BryanDocumento2 pagineNcp1 317rle Ronquillo BryanPaul AnteNessuna valutazione finora
- Oral Health DemkoDocumento27 pagineOral Health DemkoMagdalena RejmerNessuna valutazione finora
- Gmo FinalDocumento9 pagineGmo Finalapi-237602825Nessuna valutazione finora
- How To Prevent Flatulence (Aerophagy)Documento7 pagineHow To Prevent Flatulence (Aerophagy)krishnaNessuna valutazione finora
- Oils and Fats GlossaryDocumento19 pagineOils and Fats GlossaryThais Soraluz HidalgoNessuna valutazione finora
- SUPPLY SIDE West 2021Documento48 pagineSUPPLY SIDE West 2021Hebei Meishen SiraNessuna valutazione finora