Potrebbero piacerti anche
- Gastrointestinal Anatomy and Physiology: The EssentialsDa EverandGastrointestinal Anatomy and Physiology: The EssentialsJohn F. ReinusNessuna valutazione finora
- Nephrotic and Nephritic SyndromesDocumento27 pagineNephrotic and Nephritic SyndromesJoshua Smith100% (1)
- Practical Gastroenterology and Hepatology Board Review ToolkitDa EverandPractical Gastroenterology and Hepatology Board Review ToolkitKenneth R. DeVaultNessuna valutazione finora
- An Overview Of: Acute Kidney Injury (Aki: Hasan BasriDocumento22 pagineAn Overview Of: Acute Kidney Injury (Aki: Hasan BasriDz PutraNessuna valutazione finora
- Approach To HematuriaDocumento45 pagineApproach To HematuriaArun GeorgeNessuna valutazione finora
- Aplastic AnaemiaDocumento21 pagineAplastic AnaemiaAbhinav ReddyNessuna valutazione finora
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Lipid Lowering DrugsDocumento15 pagineLipid Lowering Drugsmwaithira71682Nessuna valutazione finora
- Paget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesDa EverandPaget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesNessuna valutazione finora
- Genetic Basis of Disease PMDocumento79 pagineGenetic Basis of Disease PMsunday daniel100% (1)
- Filariasis: Causes, Tests, and Treatment OptionsDa EverandFilariasis: Causes, Tests, and Treatment OptionsValutazione: 5 su 5 stelle5/5 (2)
- Synovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandSynovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Jaundice: DR: Ramy A. SamyDocumento42 pagineJaundice: DR: Ramy A. Samyoscar3spurgeonNessuna valutazione finora
- Robbins Ch. 19 The Pancreas Review QuestionsDocumento3 pagineRobbins Ch. 19 The Pancreas Review QuestionsPA2014100% (1)
- Disease of The Biliary TractDocumento7 pagineDisease of The Biliary TractMae DoctoleroNessuna valutazione finora
- A Simple Guide to Adrenal Cancer, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Adrenal Cancer, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- PATH - Acute Kidney InjuryDocumento12 paginePATH - Acute Kidney InjuryAyyaz HussainNessuna valutazione finora
- Biliary Tree LectureDocumento58 pagineBiliary Tree Lecturesgod34Nessuna valutazione finora
- Wilson S DiseaseDocumento28 pagineWilson S DiseasemichaelcylNessuna valutazione finora
- 10 EdemaDocumento23 pagine10 EdemaTalmaciu AmyNessuna valutazione finora
- For More Details Please Visit Our WebsiteDocumento25 pagineFor More Details Please Visit Our Websiteajie354Nessuna valutazione finora
- CholelithiasisDocumento6 pagineCholelithiasisLara GatbontonNessuna valutazione finora
- Presentation JaundiceDocumento49 paginePresentation JaundiceVinoth KumarNessuna valutazione finora
- Pathology of LiverDocumento15 paginePathology of Liverערין גבאריןNessuna valutazione finora
- Advances in Pathobiology and Management of Paget’s Disease of BoneDa EverandAdvances in Pathobiology and Management of Paget’s Disease of BoneSakamuri V. ReddyNessuna valutazione finora
- Renal DisordersDocumento77 pagineRenal Disorderslorelee_espaldon100% (1)
- Lymphoid NeoplasmsDocumento52 pagineLymphoid NeoplasmsAmalia Riska GNessuna valutazione finora
- Malignant Liver Tumors Undergrad 6th Year Students SharaanDocumento56 pagineMalignant Liver Tumors Undergrad 6th Year Students SharaanMohamed AhmedNessuna valutazione finora
- A Simple Guide to Acalculous Cholecystopathy, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Acalculous Cholecystopathy, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Patho SlidesDocumento46 paginePatho Slidesapi-400411160Nessuna valutazione finora
- Thalasemia and HemoglobinopathiDocumento57 pagineThalasemia and HemoglobinopathiChristan Chaputtra MaharibeNessuna valutazione finora
- UROLITHIASISDocumento25 pagineUROLITHIASISPaulo ManlangitNessuna valutazione finora
- HepatosplenomegalyDocumento52 pagineHepatosplenomegalySundar NatarajanNessuna valutazione finora
- Aspirin OverdoseDocumento3 pagineAspirin OverdoseSaputra BismaNessuna valutazione finora
- By: DR Eyad Talal: Moderator: DR I - QudaisatDocumento55 pagineBy: DR Eyad Talal: Moderator: DR I - QudaisatEyad AbdeljawadNessuna valutazione finora
- Cirrhosis Jol 2009Documento54 pagineCirrhosis Jol 2009SaaraAlleyahAlAnazi100% (1)
- Urolithiasis SeminarDocumento50 pagineUrolithiasis SeminarSiddharth GuptaNessuna valutazione finora
- Diabetes MellitusDocumento79 pagineDiabetes Mellituskhalid saifur rahman khanNessuna valutazione finora
- Sickle Cell Anemia - 27Documento42 pagineSickle Cell Anemia - 27M.AhmedNessuna valutazione finora
- Skin Path NotesDocumento15 pagineSkin Path NoteszeeathrNessuna valutazione finora
- Pathology of Digestive SystemDocumento28 paginePathology of Digestive SystemDianNursyifaRahmahNessuna valutazione finora
- Renal PathologyDocumento28 pagineRenal PathologyApril Deveras JudillaNessuna valutazione finora
- Diabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandDiabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- What Is Destroying This RBC?Documento28 pagineWhat Is Destroying This RBC?Putri Azka RinandaNessuna valutazione finora
- Fibrous Dysplasia of BoneDocumento31 pagineFibrous Dysplasia of Bonet.babyNessuna valutazione finora
- Nephrotic SyndromeDocumento34 pagineNephrotic SyndromeAnusikta PandaNessuna valutazione finora
- Acute Kidney InjuryDocumento37 pagineAcute Kidney InjuryLani BuenaventuraNessuna valutazione finora
- Endocarditis PediatricDocumento56 pagineEndocarditis Pediatricfarzzana100% (1)
- Pancoast Syndrome, (Apical Lung Cancer) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandPancoast Syndrome, (Apical Lung Cancer) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- The Liver: Dr. I Made Naris Pujawan, M.Biomed, SP - PADocumento19 pagineThe Liver: Dr. I Made Naris Pujawan, M.Biomed, SP - PAAnonymous D29e00Nessuna valutazione finora
- Haematological DisordersDocumento28 pagineHaematological DisordersSamuel kuriaNessuna valutazione finora
- Sameer Smadi MD. Amman-Jordan: Consultant HBP and Liver Transplantation SurgeonDocumento179 pagineSameer Smadi MD. Amman-Jordan: Consultant HBP and Liver Transplantation SurgeonNessreen JamalNessuna valutazione finora
- An Introduction To AnaemiaDocumento27 pagineAn Introduction To Anaemiaمجاهد إسماعيل حسن حسينNessuna valutazione finora
- Peptic Ulcer DiseaseDocumento36 paginePeptic Ulcer DiseaseRamanujam SekarNessuna valutazione finora
- 2-Acute Abdominal PainDocumento24 pagine2-Acute Abdominal Painabdalmajeed alshammaryNessuna valutazione finora
- Liver Curs 2009Documento215 pagineLiver Curs 2009Mohammad_Islam87Nessuna valutazione finora
- Morphopathology SET 16 Pathologies of The Gastrointestinal TractDocumento29 pagineMorphopathology SET 16 Pathologies of The Gastrointestinal TractMohammad_Islam87Nessuna valutazione finora
- Lecture 20 CarcinogenesisDocumento84 pagineLecture 20 CarcinogenesisMohammad_Islam87100% (1)
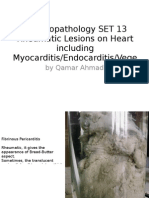
- Morphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeDocumento25 pagineMorphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeMohammad_Islam87Nessuna valutazione finora
- Morphopathology SET 15 Renal Pathologies: by Qamar AhmadDocumento25 pagineMorphopathology SET 15 Renal Pathologies: by Qamar AhmadMohammad_Islam87Nessuna valutazione finora
- Morphopathology Macroscopy (Romanian-Batch)Documento187 pagineMorphopathology Macroscopy (Romanian-Batch)Mohammad_Islam87100% (1)
- Morphopathology SET14 Respiratory Pathologies: by Qamar AhmadDocumento18 pagineMorphopathology SET14 Respiratory Pathologies: by Qamar AhmadMohammad_Islam87Nessuna valutazione finora
- ?#ry%oefr: - J4 @,8/ MryDocumento15 pagine?#ry%oefr: - J4 @,8/ MryMohammad_Islam87Nessuna valutazione finora
- Borcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocumento7 pagineBorcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87100% (1)
- Morphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadDocumento19 pagineMorphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadMohammad_Islam87Nessuna valutazione finora
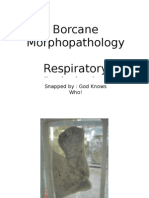
- Borcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocumento11 pagineBorcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Nessuna valutazione finora
- Borcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocumento7 pagineBorcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Nessuna valutazione finora
- Workshop 17Documento4 pagineWorkshop 17Mohammad_Islam87Nessuna valutazione finora
- Morphopatholgy Set 9 Circulatory Disturbances: by Qamar AhmadDocumento24 pagineMorphopatholgy Set 9 Circulatory Disturbances: by Qamar AhmadMohammad_Islam87Nessuna valutazione finora
- Workshop 19Documento3 pagineWorkshop 19Mohammad_Islam87Nessuna valutazione finora
- Workshop 20Documento2 pagineWorkshop 20Mohammad_Islam87Nessuna valutazione finora
- Conditions Presenting With Abdominal PainDocumento69 pagineConditions Presenting With Abdominal PainaimanNessuna valutazione finora
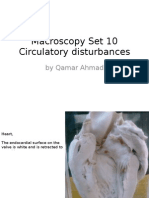
- Macroscopy Set 10 Circulatory Disturbances: by Qamar AhmadDocumento55 pagineMacroscopy Set 10 Circulatory Disturbances: by Qamar AhmadMohammad_Islam87Nessuna valutazione finora
- Physical Signs of The AbdomenDocumento93 paginePhysical Signs of The AbdomenaimanNessuna valutazione finora
- Morphopathology Set 8 Melanocytic Tumors: by Qamar AhmadDocumento54 pagineMorphopathology Set 8 Melanocytic Tumors: by Qamar AhmadMohammad_Islam87Nessuna valutazione finora
- Morphopathology Set 11 Atherosclerosis and Other Cardiaovascular DisordersDocumento21 pagineMorphopathology Set 11 Atherosclerosis and Other Cardiaovascular DisordersMohammad_Islam87Nessuna valutazione finora
- Workshop 18Documento4 pagineWorkshop 18Mohammad_Islam87Nessuna valutazione finora
- STOMACCURS2Documento12 pagineSTOMACCURS2Mohammad_Islam87Nessuna valutazione finora
- Peptic Ulcer DiseaseDocumento54 paginePeptic Ulcer DiseaseMohammad_Islam87Nessuna valutazione finora
- Stomach - GastritisDocumento22 pagineStomach - GastritisaimanNessuna valutazione finora
- Examination of AbdomenDocumento41 pagineExamination of AbdomenMohammad_Islam87Nessuna valutazione finora
- Lung FlukesDocumento23 pagineLung FlukesGelli LebinNessuna valutazione finora
- Material Safety Data Sheet: 1. Product and Manufacturer IdentityDocumento8 pagineMaterial Safety Data Sheet: 1. Product and Manufacturer IdentityCamilo AquinoNessuna valutazione finora
- Medicinal Flora in Holy QuranDocumento16 pagineMedicinal Flora in Holy QuranMuhammad Zakiy FadlullahNessuna valutazione finora
- Genetic Disorder Webquest ArtifactDocumento13 pagineGenetic Disorder Webquest Artifactapi-582653189Nessuna valutazione finora
- MCU 2021 The Ventilator Book 3rd EditionDocumento280 pagineMCU 2021 The Ventilator Book 3rd EditionAlvaro Estupiñan100% (2)
- QBANKDocumento38 pagineQBANKsbarolia2673% (11)
- Heart DiseaseDocumento26 pagineHeart DiseaseJulia MarieNessuna valutazione finora
- Maintenance Fluid Therapy in ChildrenDocumento4 pagineMaintenance Fluid Therapy in ChildrenNicole_0Nessuna valutazione finora
- Esmr 2Documento1 paginaEsmr 2Martina FitriaNessuna valutazione finora
- Abdurasad NSO HemoglucotestDocumento5 pagineAbdurasad NSO HemoglucotestNader AbdurasadNessuna valutazione finora
- Ppz3o - Unit 1Documento136 paginePpz3o - Unit 1api-266151891Nessuna valutazione finora
- Endocrine DisordersDocumento106 pagineEndocrine DisordersMansur MuhammadNessuna valutazione finora
- Common - CardioDocumento91 pagineCommon - CardioHanadi UmhanayNessuna valutazione finora
- NCMB312 RLE-Burn Injuries-Group 3Documento56 pagineNCMB312 RLE-Burn Injuries-Group 3Maica LectanaNessuna valutazione finora
- Digestive Care - ADVEN BIOTECH GURGAONDocumento7 pagineDigestive Care - ADVEN BIOTECH GURGAONmljaininsulationNessuna valutazione finora
- Family Planning Association of India Madurai BranchDocumento12 pagineFamily Planning Association of India Madurai BranchValarmathiNessuna valutazione finora
- Alcohol WithdrawalDocumento28 pagineAlcohol WithdrawalMohammed AlshamsiNessuna valutazione finora
- Definition of Sepsis Matot 2001Documento1 paginaDefinition of Sepsis Matot 2001Flavia Oliveira PampolhaNessuna valutazione finora
- The Neuropsychiatry of EpilepsyDocumento361 pagineThe Neuropsychiatry of Epilepsypablo_zabala100% (3)
- Assignment On Unconciousness: Subject:-Advanced Nursing PracticeDocumento15 pagineAssignment On Unconciousness: Subject:-Advanced Nursing PracticeShaells JoshiNessuna valutazione finora
- Why Do Adolescents Start Smoking?: Name: Tommy-Lee Richards Subject: HSB SBADocumento55 pagineWhy Do Adolescents Start Smoking?: Name: Tommy-Lee Richards Subject: HSB SBAcruze0% (1)
- Essay BeckDocumento12 pagineEssay BeckSusana PoncianoNessuna valutazione finora
- Clinical Appearance of Oral Lesions in Bronchial Asthma Patients Using Inhalation DrugDocumento7 pagineClinical Appearance of Oral Lesions in Bronchial Asthma Patients Using Inhalation DrugDenna Idryareza AugustyanaNessuna valutazione finora
- Government Initiatives in Health and Nutrition: Vinod PaulDocumento29 pagineGovernment Initiatives in Health and Nutrition: Vinod PaulMani KandanNessuna valutazione finora
- Dental Consent FormDocumento2 pagineDental Consent Formkoshimannu100% (1)
- Diarrhea in ChildrenDocumento23 pagineDiarrhea in ChildrenSudeshna YadavNessuna valutazione finora
- General Dermatology NotesDocumento6 pagineGeneral Dermatology NotesPenny_Teoh_3451Nessuna valutazione finora
- SIC (Carpio, Kurt Andrew)Documento5 pagineSIC (Carpio, Kurt Andrew)Kurt Andrew CarpioNessuna valutazione finora
- 12 Physiology EyelidsDocumento119 pagine12 Physiology EyelidsYoussefNessuna valutazione finora
- 11 FNSDDocumento16 pagine11 FNSDVamsi VasishtNessuna valutazione finora