Potrebbero piacerti anche
- Lecture 20 CarcinogenesisDocumento84 pagineLecture 20 CarcinogenesisMohammad_Islam87100% (1)
- AnaemiaDocumento83 pagineAnaemiaMohammad_Islam87100% (2)
- Physiopathology SyllabusDocumento1 paginaPhysiopathology SyllabusMohammad_Islam87Nessuna valutazione finora
- Lecture 18 Upper Digestive DiseasesDocumento63 pagineLecture 18 Upper Digestive DiseasesMohammad_Islam87Nessuna valutazione finora
- The BreastDocumento72 pagineThe BreastMohammad_Islam87Nessuna valutazione finora
- Plastic SurgeryDocumento11 paginePlastic SurgeryMohammad_Islam87Nessuna valutazione finora
- The LymphomasDocumento46 pagineThe LymphomasMohammad_Islam87Nessuna valutazione finora
- Curst Um Abd EnglDocumento10 pagineCurst Um Abd EnglMohammad_Islam87Nessuna valutazione finora
- Lecture 17 DiabetesDocumento51 pagineLecture 17 DiabetesMohammad_Islam87Nessuna valutazione finora
- Morphopathology SET 16 Pathologies of The Gastrointestinal TractDocumento29 pagineMorphopathology SET 16 Pathologies of The Gastrointestinal TractMohammad_Islam87Nessuna valutazione finora
- Abdominal HerniaeDocumento66 pagineAbdominal HerniaeMohammad_Islam87Nessuna valutazione finora
- Liver Curs 2009Documento215 pagineLiver Curs 2009Mohammad_Islam87Nessuna valutazione finora
- Borcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocumento7 pagineBorcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Nessuna valutazione finora
- Pharmacology Lecture 12-5-2009, OpiodsDocumento18 paginePharmacology Lecture 12-5-2009, OpiodsMohammad_Islam87Nessuna valutazione finora
- Morphopathology SET 15 Renal Pathologies: by Qamar AhmadDocumento25 pagineMorphopathology SET 15 Renal Pathologies: by Qamar AhmadMohammad_Islam87Nessuna valutazione finora
- Morphopathology Macroscopy (Romanian-Batch)Documento187 pagineMorphopathology Macroscopy (Romanian-Batch)Mohammad_Islam87100% (1)
- Pharmacology Lecture 19-5-2009, NSAIDSDocumento19 paginePharmacology Lecture 19-5-2009, NSAIDSMohammad_Islam87Nessuna valutazione finora
- Morphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadDocumento19 pagineMorphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadMohammad_Islam87Nessuna valutazione finora
- Morphopathology SET14 Respiratory Pathologies: by Qamar AhmadDocumento18 pagineMorphopathology SET14 Respiratory Pathologies: by Qamar AhmadMohammad_Islam87Nessuna valutazione finora
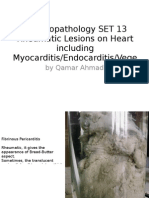
- Morphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeDocumento25 pagineMorphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeMohammad_Islam87Nessuna valutazione finora
- Borcane TumorDocumento14 pagineBorcane TumorMohammad_Islam87Nessuna valutazione finora
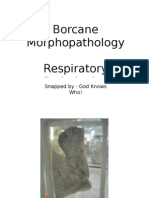
- Borcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocumento11 pagineBorcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Nessuna valutazione finora
- ?#ry%oefr: - J4 @,8/ MryDocumento15 pagine?#ry%oefr: - J4 @,8/ MryMohammad_Islam87Nessuna valutazione finora
- Pharmacology Lecture Diuretic Agents (High Quality)Documento15 paginePharmacology Lecture Diuretic Agents (High Quality)Mohammad_Islam87Nessuna valutazione finora
- Borcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocumento7 pagineBorcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87100% (1)
- Workshop 20Documento2 pagineWorkshop 20Mohammad_Islam87Nessuna valutazione finora
- Workshop 19Documento3 pagineWorkshop 19Mohammad_Islam87Nessuna valutazione finora
- Pharmacology Lecture 5-5-2009Documento15 paginePharmacology Lecture 5-5-2009Mohammad_Islam87Nessuna valutazione finora
- Conditions Presenting With Abdominal PainDocumento69 pagineConditions Presenting With Abdominal PainaimanNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Drug Study 4 SatDocumento1 paginaDrug Study 4 SatHayley Ace RilloNessuna valutazione finora
- RektokelDocumento13 pagineRektokelIntan PermataNessuna valutazione finora
- Name: Age: Sex: Place: Occupation: Chief ComplaintsDocumento3 pagineName: Age: Sex: Place: Occupation: Chief ComplaintsmuniNessuna valutazione finora
- Patient Medical RecordDocumento1 paginaPatient Medical RecordKyla Barrera TabungarNessuna valutazione finora
- Importance of WaterDocumento10 pagineImportance of WaterKristelCruzCayetanoNessuna valutazione finora
- Assessment Constipation PDFDocumento6 pagineAssessment Constipation PDFDennis CobbNessuna valutazione finora
- Matary Cases 2013Documento153 pagineMatary Cases 2013Raouf Ra'fat Soliman100% (10)
- FGIDsDocumento37 pagineFGIDsBenjamin TennysonNessuna valutazione finora
- Practical Prescriber PDFDocumento515 paginePractical Prescriber PDFGandhi Lanka100% (2)
- Review: Treatment of Constipation in Older PeopleDocumento8 pagineReview: Treatment of Constipation in Older PeopleMohd ZulAmirulNessuna valutazione finora
- KonstipasivgfvhDocumento16 pagineKonstipasivgfvhrharaNessuna valutazione finora
- Case Presentation - HerniaDocumento19 pagineCase Presentation - HerniaElvin Louie Lisondra100% (1)
- Gastrointestinal DiseasesDocumento9 pagineGastrointestinal DiseasesJeraLdine HÜfanoNessuna valutazione finora
- Fdar Prcedure EndorsmentDocumento9 pagineFdar Prcedure EndorsmentFelipe MeranoNessuna valutazione finora
- FHN - Nursing Care Plan Constipation)Documento3 pagineFHN - Nursing Care Plan Constipation)blahniksNessuna valutazione finora
- Constipation Risk Assessment ToolDocumento2 pagineConstipation Risk Assessment ToolAnggie Anggriyana100% (1)
- 300 Nle ExamDocumento13 pagine300 Nle Examyage1322100% (1)
- PATANJALI AYURVEDA, Research ReportDocumento42 paginePATANJALI AYURVEDA, Research ReportPranav DattaNessuna valutazione finora
- Constipation On A Low-Carb DietDocumento11 pagineConstipation On A Low-Carb DietYet AnotherNessuna valutazione finora
- Nursing Diagnoses & Interventions for Schizophrenia ClientDocumento6 pagineNursing Diagnoses & Interventions for Schizophrenia ClientJesselle LasernaNessuna valutazione finora
- Drugs Affecting Gastrointestinal Motility Drugs Affecting Gastrointestinal MotilityDocumento34 pagineDrugs Affecting Gastrointestinal Motility Drugs Affecting Gastrointestinal MotilityJojo JustoNessuna valutazione finora
- Hirschsprung DiseaseDocumento13 pagineHirschsprung Diseaseganesh reddyNessuna valutazione finora
- NCLEX Test ReviewDocumento7 pagineNCLEX Test ReviewPhuong Tran100% (1)
- Acute AbdomenDocumento31 pagineAcute AbdomenTriono AssamsulNessuna valutazione finora
- Bates' Guide To Physical Examination and History Taking, 12th EditionDocumento10 pagineBates' Guide To Physical Examination and History Taking, 12th EditionmanesNessuna valutazione finora
- Drug StudyDocumento7 pagineDrug StudyKarol Ann RodriguezNessuna valutazione finora
- Cues/Needs Nursing Diagnosis Scientific Explanation Goals and Objectives Nursing Intervention Rationale Evaluation Short Term Independent Short TermDocumento3 pagineCues/Needs Nursing Diagnosis Scientific Explanation Goals and Objectives Nursing Intervention Rationale Evaluation Short Term Independent Short TermLatrell GelacioNessuna valutazione finora
- Treating Constipation and Anal Stenosis in a 7-Month-OldDocumento35 pagineTreating Constipation and Anal Stenosis in a 7-Month-OldAbigail CruzNessuna valutazione finora
- Dr. M.S. Shamol Fcps (Medicine) : C O T S N I P A T I O NDocumento20 pagineDr. M.S. Shamol Fcps (Medicine) : C O T S N I P A T I O NiwanNessuna valutazione finora
- Susah BabDocumento45 pagineSusah BabaghniaNessuna valutazione finora