Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- PorphyriaDocumento10 paginePorphyriaDeepankar Srigyan0% (1)
- Acute Abdomen and Peptic UlcerDocumento69 pagineAcute Abdomen and Peptic UlcerDeepankar SrigyanNessuna valutazione finora
- Hodgkin's LymphomaDocumento10 pagineHodgkin's LymphomaDeepankar SrigyanNessuna valutazione finora
- Vaccinations Are Offered To All Children ToDocumento1 paginaVaccinations Are Offered To All Children ToDeepankar SrigyanNessuna valutazione finora
- Phytoestrogens and Breast CancerDocumento6 paginePhytoestrogens and Breast CancerDeepankar SrigyanNessuna valutazione finora
- Disease Incubation PeriodDocumento1 paginaDisease Incubation PeriodDeepankar SrigyanNessuna valutazione finora
- Drugs in PregnancyDocumento2 pagineDrugs in PregnancyDeepankar SrigyanNessuna valutazione finora
- Phytoestrogens: Phytoestrogens, Sometimes Called "Dietary Estrogens", Are A Diverse Group of Naturally OccurringDocumento5 paginePhytoestrogens: Phytoestrogens, Sometimes Called "Dietary Estrogens", Are A Diverse Group of Naturally OccurringDeepankar SrigyanNessuna valutazione finora
- Phytoestrogens: - by Deepankar SrigyanDocumento13 paginePhytoestrogens: - by Deepankar SrigyanDeepankar SrigyanNessuna valutazione finora
- Evidence Based MedicinesDocumento9 pagineEvidence Based MedicinesDeepankar SrigyanNessuna valutazione finora
- Hemolytic AnemiasDocumento25 pagineHemolytic AnemiasDeepankar SrigyanNessuna valutazione finora
- Macrocytic AnemiasDocumento28 pagineMacrocytic AnemiasDeepankar SrigyanNessuna valutazione finora
- Ancient India's Contribution To Medical ScienceDocumento14 pagineAncient India's Contribution To Medical ScienceDeepankar SrigyanNessuna valutazione finora
- Heat Stable and Light Sensitive Vitamin KDocumento2 pagineHeat Stable and Light Sensitive Vitamin KDeepankar SrigyanNessuna valutazione finora
- Fetal Birth InjuriesDocumento104 pagineFetal Birth InjuriesDeepankar SrigyanNessuna valutazione finora
- AttitudeDocumento9 pagineAttitudewhereisthebody100% (13)
- Prostate CancerDocumento14 pagineProstate CancerDeepankar Srigyan100% (1)
- Blood DiseasesDocumento42 pagineBlood DiseasesDeepankar SrigyanNessuna valutazione finora
- How To Say I Love You in 100 LanguagesDocumento4 pagineHow To Say I Love You in 100 LanguagesRosca MariusNessuna valutazione finora
- Breast CancerDocumento7 pagineBreast CancerDeepankar Srigyan100% (1)
- HepatitisDocumento10 pagineHepatitisDeepankar SrigyanNessuna valutazione finora
- Pediatric Patient Case History 2009Documento11 paginePediatric Patient Case History 2009Deepankar Srigyan100% (1)
- Three EnemiesDocumento1 paginaThree EnemiesDeepankar SrigyanNessuna valutazione finora
- Trematodes and RicktesiosisDocumento2 pagineTrematodes and RicktesiosisDeepankar SrigyanNessuna valutazione finora
- Bacterial InfectionsDocumento2 pagineBacterial InfectionsDeepankar SrigyanNessuna valutazione finora
- ImmunityDocumento2 pagineImmunityDeepankar Srigyan100% (1)
- Amebiasis (Ant Hroponosis) (20) Forms: E. HistolyticaDocumento7 pagineAmebiasis (Ant Hroponosis) (20) Forms: E. HistolyticaDeepankar SrigyanNessuna valutazione finora
- NewYear PpsDocumento1 paginaNewYear PpsDeepankar SrigyanNessuna valutazione finora
- Public Health Project of India 2008Documento143 paginePublic Health Project of India 2008Deepankar Srigyan80% (5)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- ECG Rounds May 201Documento39 pagineECG Rounds May 201CetriseNessuna valutazione finora
- CALIXRO, LJ NARRATIVE Ventricular Septal DefectDocumento2 pagineCALIXRO, LJ NARRATIVE Ventricular Septal DefectKim SunooNessuna valutazione finora
- Achieving Excellence in The OSCE Part 1Documento409 pagineAchieving Excellence in The OSCE Part 1Sultan AlexandruNessuna valutazione finora
- Arie Bachtiar Dwitaryo Bagian Kardiologi Dan Kedokteran Vaskular FK. UNDIP / RS. Dr. Kariadi SemarangDocumento34 pagineArie Bachtiar Dwitaryo Bagian Kardiologi Dan Kedokteran Vaskular FK. UNDIP / RS. Dr. Kariadi SemarangSebastiana Ratih LefebvreNessuna valutazione finora
- Basic Electrocardiography NewDocumento25 pagineBasic Electrocardiography NewMoh Arif KurniawanNessuna valutazione finora
- Chapter 22 The First Heart SoundDocumento5 pagineChapter 22 The First Heart SoundAbhilash ReddyNessuna valutazione finora
- ACLS (Notes) (Printable)Documento2 pagineACLS (Notes) (Printable)mike_germain1172Nessuna valutazione finora
- Pem. Cardiovaskular Dr. MulyadiDocumento195 paginePem. Cardiovaskular Dr. MulyadiBettry Ahmad100% (1)
- Ecg - AclsDocumento338 pagineEcg - AclsPete Cobra CobraitiNessuna valutazione finora
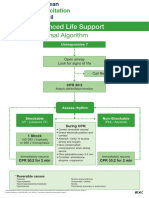
- Advanced Life Support - A0 PDFDocumento1 paginaAdvanced Life Support - A0 PDFiulia-uroNessuna valutazione finora
- Diastolic Murmurs: Classification, Mechanisms and CausesDocumento47 pagineDiastolic Murmurs: Classification, Mechanisms and CausesHenry Franz Flores NicolásNessuna valutazione finora
- Daftar Pustaka ImaDocumento2 pagineDaftar Pustaka ImaDesrina PungkyNessuna valutazione finora
- AmiodaroneDocumento2 pagineAmiodaroneEmmil BernardoNessuna valutazione finora
- Case 7 - (Muhamad Adi) FirehawkDocumento11 pagineCase 7 - (Muhamad Adi) FirehawkMochamad Rizky HendiperdanaNessuna valutazione finora
- Ecg Tutorial PDFDocumento82 pagineEcg Tutorial PDFpacpacpac123Nessuna valutazione finora
- ECG Characteristics and Management of Cardiac RhythmsDocumento6 pagineECG Characteristics and Management of Cardiac RhythmsJeffrey Viernes100% (1)
- ECG Workshop 2006Documento15 pagineECG Workshop 2006Eggi ErlanggaNessuna valutazione finora
- Bos Specialty Assignment Cardiology-AmbroseDocumento11 pagineBos Specialty Assignment Cardiology-Ambroseapi-396965096Nessuna valutazione finora
- Pathophysiology of Cardiogenic Pulmonary EdemaDocumento13 paginePathophysiology of Cardiogenic Pulmonary EdemaIrina DuceacNessuna valutazione finora
- Ajmaline and its derivatives: a review of neurological, hematological, and organ-related adverse effectsDocumento2 pagineAjmaline and its derivatives: a review of neurological, hematological, and organ-related adverse effectsKmilo VargasNessuna valutazione finora
- ArrthymiasDocumento11 pagineArrthymiasSyafiq AbeNessuna valutazione finora
- Compact ECG Arrhythmia SimulatorDocumento2 pagineCompact ECG Arrhythmia SimulatorismailshajjiNessuna valutazione finora
- UQU 2nd Edition of SLE Questions 2013Documento395 pagineUQU 2nd Edition of SLE Questions 2013ztijarhura90% (10)
- Penyakit Jantung KongenitalDocumento30 paginePenyakit Jantung KongenitalrintiikNessuna valutazione finora
- MurmursDocumento3 pagineMurmursSijo SunnyNessuna valutazione finora
- Macleods Clinical Examination 14th Edition-57-91Documento36 pagineMacleods Clinical Examination 14th Edition-57-91bv2328002Nessuna valutazione finora
- Management of Cardiac ArrestDocumento40 pagineManagement of Cardiac ArrestMark Francis NaniaNessuna valutazione finora
- Basic ECG ReadingDocumento41 pagineBasic ECG ReadingBenj100% (3)
- ACLS Rhythms Cheat SheetDocumento21 pagineACLS Rhythms Cheat SheetSisca MetasariNessuna valutazione finora
- DYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDocumento3 pagineDYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDarell M. Book100% (1)