Potrebbero piacerti anche
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Hiatus Hernia - Chinese Herbs, Chinese Medicine, AcupunctureDocumento6 pagineHiatus Hernia - Chinese Herbs, Chinese Medicine, AcupunctureCarlCordNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- MLN CatalogDocumento24 pagineMLN CatalogLhingboi100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Benign Prostatic Hyperplasia - BPH - Pathophysiology - Schematic DiagramDocumento2 pagineBenign Prostatic Hyperplasia - BPH - Pathophysiology - Schematic DiagramSimran JosanNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Electronic Edge ExampleDocumento138 pagineElectronic Edge Examplezarrin77Nessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- 3.chronic IllnessesDocumento51 pagine3.chronic IllnessesJonalyn EtongNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- List of Notified Bodies Under Directive - 93-42 EEC Medical DevicesDocumento332 pagineList of Notified Bodies Under Directive - 93-42 EEC Medical DevicesJamal MohamedNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Microbiologist: 3.1.5 Isolation & Gram StainingDocumento5 pagineMicrobiologist: 3.1.5 Isolation & Gram Stainingapi-534896073Nessuna valutazione finora
- Therapeutic Classification of DrugsDocumento4 pagineTherapeutic Classification of Drugslyn lynNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Neutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisDocumento7 pagineNeutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisHamza AhmedNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Sri Ramachandra University Application-09Documento5 pagineSri Ramachandra University Application-09Mohammed RaziNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Case Report Child AbuseDocumento7 pagineCase Report Child AbuseEuis MayaNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Domain 2 Public Health AnnotationsDocumento9 pagineDomain 2 Public Health AnnotationsjkdanielesNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Angio EdemaDocumento172 pagineAngio Edemaalma23roNessuna valutazione finora
- Enfant Cheri Study Centre, Inc. 4 Mid Quarter Examination T.L.E. 7Documento2 pagineEnfant Cheri Study Centre, Inc. 4 Mid Quarter Examination T.L.E. 7AR Joy Gardiola TampilNessuna valutazione finora
- Possible Interview Questions For NursesDocumento32 paginePossible Interview Questions For NursesElisabeta Ivan75% (4)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- 2018 Jordanian Conference BookletDocumento51 pagine2018 Jordanian Conference BookletAurelian Corneliu MoraruNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Pediatrics Respiratory Emergencies: Samuel HarminDocumento41 paginePediatrics Respiratory Emergencies: Samuel HarminUmbu ArnoldNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Upper Extremity Reconstruction: Surgical SolutionsDocumento16 pagineUpper Extremity Reconstruction: Surgical Solutionsapi-488115640Nessuna valutazione finora
- Egerton University: Office of The Registrar (Academic Affairs)Documento8 pagineEgerton University: Office of The Registrar (Academic Affairs)Deb0% (1)
- Company Profile Indo Medika InternationalDocumento12 pagineCompany Profile Indo Medika InternationalshavinravizaNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Mann Assessment of Swallowing AbilityDocumento9 pagineMann Assessment of Swallowing Abilityluca bastianiNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Cognium Syrup Pharmacological Properties SummaryDocumento6 pagineCognium Syrup Pharmacological Properties SummaryMitzi MitchellNessuna valutazione finora
- Retinopathy of PrematurityDocumento15 pagineRetinopathy of Prematuritymarissa ulkhairNessuna valutazione finora
- SAM's Drugs GuideDocumento499 pagineSAM's Drugs Guideصباح عباس الساعديNessuna valutazione finora
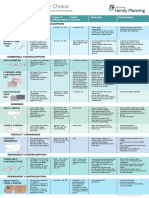
- Contraception Options in New ZealandDocumento2 pagineContraception Options in New ZealandStuff NewsroomNessuna valutazione finora
- Jurnal Kel. 11-12Documento20 pagineJurnal Kel. 11-12Rinda YulianaNessuna valutazione finora
- Pediatric Blunt TraumaDocumento10 paginePediatric Blunt TraumaBernard100% (1)
- Osteomyelitis: Dr. Sushil PaudelDocumento107 pagineOsteomyelitis: Dr. Sushil PaudelPryta WidyaningrumNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Reflective Essay Samantha JohnsonDocumento5 pagineReflective Essay Samantha Johnsonapi-329945753Nessuna valutazione finora
- Tumors of External EarDocumento10 pagineTumors of External Earsavin1996100% (2)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)