Potrebbero piacerti anche
- Grief and LossDocumento38 pagineGrief and LossPrince ZioNessuna valutazione finora
- Coping With LossDocumento5 pagineCoping With LossRaman SamraoNessuna valutazione finora
- Greg Bocchino - Grief and Loss PowerpointDocumento26 pagineGreg Bocchino - Grief and Loss PowerpointDocStevensNessuna valutazione finora
- Loss, Death, and Grieving: Nursing Fundamentals Nurs B20Documento19 pagineLoss, Death, and Grieving: Nursing Fundamentals Nurs B20rinkuNessuna valutazione finora
- The Dying Persons Bill of RightsDocumento2 pagineThe Dying Persons Bill of RightsJm OpolintoNessuna valutazione finora
- Grief, Loss, Death and DyingDocumento47 pagineGrief, Loss, Death and DyingRaquel M. MendozaNessuna valutazione finora
- Death and DyingDocumento52 pagineDeath and DyingKaren HernandezNessuna valutazione finora
- Developmental PsychologyDocumento9 pagineDevelopmental PsychologyAengewycaNessuna valutazione finora
- Loss, Grief, and DyingDocumento17 pagineLoss, Grief, and Dyingmazenalayed100% (2)
- Coping With LossDocumento23 pagineCoping With LossRuby Sri100% (2)
- Psychiatric Nursing Handout 09-10 FCDocumento38 paginePsychiatric Nursing Handout 09-10 FCAlvin Flores AbalosNessuna valutazione finora
- Endofthelifeofa Person .: Dying & Death Definition of Death: in Simple Words Death Can Be Defined AsDocumento2 pagineEndofthelifeofa Person .: Dying & Death Definition of Death: in Simple Words Death Can Be Defined AskaranNessuna valutazione finora
- Death and DyingDocumento56 pagineDeath and DyingManish Kumar100% (1)
- Death & DyingDocumento28 pagineDeath & DyingTom TsouNessuna valutazione finora
- Grief and Loss, Dying/ DeadDocumento5 pagineGrief and Loss, Dying/ DeadAaron ConstantinoNessuna valutazione finora
- Grief, Stages of Grief and Grief ProcessDocumento6 pagineGrief, Stages of Grief and Grief ProcessEdrea Aquino Mendez100% (2)
- The Transmigration of SoulsDocumento146 pagineThe Transmigration of Soulskikkuri13100% (3)
- Psychotherapy With The Dying PatientDocumento21 paginePsychotherapy With The Dying PatientAdelina RotaruNessuna valutazione finora
- A Psychological and Philosophical Understanding of Death - An AnaDocumento60 pagineA Psychological and Philosophical Understanding of Death - An AnanaomiNessuna valutazione finora
- TOPIC: The Structure of Personality Client-Centered (Carl Rogers) DISCUSSANT: Mary Ann S. Ariente MAED ASDocumento1 paginaTOPIC: The Structure of Personality Client-Centered (Carl Rogers) DISCUSSANT: Mary Ann S. Ariente MAED ASApril Loren Vinson HomenaNessuna valutazione finora
- Inflammatory ResponseDocumento7 pagineInflammatory Responseᵇᵅᵇᵞ Anden GonzagaNessuna valutazione finora
- End of Life BrochureDocumento32 pagineEnd of Life Brochurekatification67% (3)
- Ego Defense MechanismDocumento52 pagineEgo Defense Mechanismmac_rymrt100% (3)
- Analisis Jurnal End of Life-Tedi&saidDocumento5 pagineAnalisis Jurnal End of Life-Tedi&saidYulia JuniartiNessuna valutazione finora
- Person-Centered Therapy Application and PDFDocumento14 paginePerson-Centered Therapy Application and PDFAHMED KHAN100% (1)
- Analytic: Girl, InterruptedDocumento3 pagineAnalytic: Girl, InterruptedDenise NicoleNessuna valutazione finora
- The Stages of Grief: "If Only" Statements in Attempt To Negotiate An Alternate RealityDocumento2 pagineThe Stages of Grief: "If Only" Statements in Attempt To Negotiate An Alternate RealityJM Balane100% (1)
- Mood DisordersDocumento15 pagineMood DisordersFranco RazonNessuna valutazione finora
- Szasz - The Myth of Mental IllnessDocumento6 pagineSzasz - The Myth of Mental IllnessnukkgetNessuna valutazione finora
- Homelessness Older AdultsDocumento10 pagineHomelessness Older AdultsGeraldine Lucero100% (1)
- Stages HealingDocumento13 pagineStages Healingmanish soni100% (1)
- Spiritual NCPDocumento6 pagineSpiritual NCPMaricel R. ManabatNessuna valutazione finora
- ThanatologyDocumento37 pagineThanatologyMadalina DiacNessuna valutazione finora
- Anger VsDocumento6 pagineAnger VsHope LeeNessuna valutazione finora
- BBC - Ethics - Euthanasia - Anti-Euthanasia Arguments PDFDocumento9 pagineBBC - Ethics - Euthanasia - Anti-Euthanasia Arguments PDFMijail La TorreNessuna valutazione finora
- End of Life CareDocumento12 pagineEnd of Life CaregerajassoNessuna valutazione finora
- Death and DyingDocumento63 pagineDeath and DyingJoy Pasong100% (1)
- Elderly, Death DyingDocumento74 pagineElderly, Death DyingAmy100% (1)
- Theories of Development: Early Childhood)Documento3 pagineTheories of Development: Early Childhood)Sofia Marie GalendezNessuna valutazione finora
- End of Life IssuesDocumento35 pagineEnd of Life IssuesJeffrey RamosNessuna valutazione finora
- The Theory of Nursing As CaringDocumento3 pagineThe Theory of Nursing As CaringAnj Perez Bondoc0% (1)
- Gerontological NursingDocumento422 pagineGerontological Nursingcheenapberber100% (1)
- Rape Trauma SyndromeDocumento3 pagineRape Trauma SyndromePD11Nessuna valutazione finora
- Existential Therapy ActivityDocumento3 pagineExistential Therapy ActivityMaria Isabel CornelioNessuna valutazione finora
- Basic Nursing:Foundations of Skills & Concepts: Loss, Grief, and DeathDocumento27 pagineBasic Nursing:Foundations of Skills & Concepts: Loss, Grief, and DeathEdwin Delos Reyes AbuNessuna valutazione finora
- A Dynamic Group For The ElderlyDocumento12 pagineA Dynamic Group For The ElderlyjuaromerNessuna valutazione finora
- Grief, Mourning and BereavementDocumento5 pagineGrief, Mourning and BereavementDoc Prince Caballero100% (1)
- Maternal & Child Health CareDocumento209 pagineMaternal & Child Health CareAhsan Ul Kayum Bhuiyan100% (1)
- Bipolar 1Documento43 pagineBipolar 1rtishaiiNessuna valutazione finora
- Maladaptive Patterns of BehaviorDocumento97 pagineMaladaptive Patterns of BehaviorKimTot OctavianoNessuna valutazione finora
- Cognitive DisorderDocumento72 pagineCognitive DisorderJamal P. AlawiyaNessuna valutazione finora
- Chapter 10 Grief and LossDocumento6 pagineChapter 10 Grief and LossCatia FernandesNessuna valutazione finora
- End of Life CareDocumento80 pagineEnd of Life CareRakesh MohanNessuna valutazione finora
- Mod 1 CONCEPT OF HOSPICE-PALLIATIVE CARE, DEATH and DYINGDocumento3 pagineMod 1 CONCEPT OF HOSPICE-PALLIATIVE CARE, DEATH and DYINGJorese Hannah VictorinoNessuna valutazione finora
- Submitted By:: Madrio, Stephanne S. Uy, Jesamae Garcia, Nheriza Sarip, Ahmad M. Mr. Sherwin L. CabanletDocumento8 pagineSubmitted By:: Madrio, Stephanne S. Uy, Jesamae Garcia, Nheriza Sarip, Ahmad M. Mr. Sherwin L. CabanletjesamaeuNessuna valutazione finora
- PSYCH - Psych Emegencies 3rdDocumento42 paginePSYCH - Psych Emegencies 3rdapi-38560510% (1)
- Religious Practices Associated With Death and DyingDocumento6 pagineReligious Practices Associated With Death and DyingSonny MadambaNessuna valutazione finora
- Lesson 7 - Organ TransplantationDocumento14 pagineLesson 7 - Organ TransplantationJosee100% (1)
- Uterine CancerDocumento20 pagineUterine CancerAjurs UrsabiaNessuna valutazione finora
- Care of Terminally Ill Set 1Documento27 pagineCare of Terminally Ill Set 1saranya amuNessuna valutazione finora
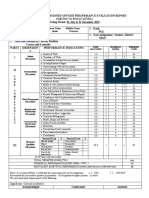
- Ratee's Name Last Name, Given Name Middle Name Galvez Jessie PanaresDocumento2 pagineRatee's Name Last Name, Given Name Middle Name Galvez Jessie PanaresMeredith GalvezNessuna valutazione finora
- HBO Individual Differences, Mental Ability, and PersonalityDocumento50 pagineHBO Individual Differences, Mental Ability, and PersonalityMeredith GalvezNessuna valutazione finora
- Challenges of TechnologyDocumento19 pagineChallenges of TechnologyMeredith GalvezNessuna valutazione finora
- Factors Affecting SleepDocumento19 pagineFactors Affecting SleepMeredith GalvezNessuna valutazione finora
- Advanced Cardiovascular Life Support in Adults (ACLS) : SubtitleDocumento30 pagineAdvanced Cardiovascular Life Support in Adults (ACLS) : SubtitleMohamad El SharNessuna valutazione finora
- Global Mental Health StudyDocumento37 pagineGlobal Mental Health StudyAustin DeneanNessuna valutazione finora
- Yes We CanDocumento3 pagineYes We CanSpeech & Language Therapy in PracticeNessuna valutazione finora
- Let'S Dive Deeply!: Discussion Points: Read The Case Scenario and Relate It To The TheoryDocumento1 paginaLet'S Dive Deeply!: Discussion Points: Read The Case Scenario and Relate It To The TheoryAnn Mariz DominguezNessuna valutazione finora
- Regula - Suture Products and Techniques What To Use, Where, and Why - 2015Documento14 pagineRegula - Suture Products and Techniques What To Use, Where, and Why - 2015Ana MariaNessuna valutazione finora
- 2 - GFSI Overview One Pager 1Documento2 pagine2 - GFSI Overview One Pager 1Diego GordoNessuna valutazione finora
- Chapter 3 The Molecules of CellsDocumento5 pagineChapter 3 The Molecules of Cellsmzunl25476Nessuna valutazione finora
- PolicyDocumento5 paginePolicySriharsha ReddyNessuna valutazione finora
- Explanatory ModelDocumento6 pagineExplanatory Modeljagdish_vankarNessuna valutazione finora
- Application FormDocumento3 pagineApplication FormSandeepSalagalaNessuna valutazione finora
- Generalized Anxiety Disorder Case Study 2017Documento4 pagineGeneralized Anxiety Disorder Case Study 2017Pratik SinghNessuna valutazione finora
- Quiz With Ans CHap 7 8 10 11Documento9 pagineQuiz With Ans CHap 7 8 10 11Junaid Khan Afridi100% (1)
- Final Panguru and Wider Community Development Report - MEA Limited PDFDocumento9 pagineFinal Panguru and Wider Community Development Report - MEA Limited PDFKaye-Maree DunnNessuna valutazione finora
- Zimbabwe's Economic Crisis Driving Homeless Boys Into Illegal Gay Sex TradeDocumento4 pagineZimbabwe's Economic Crisis Driving Homeless Boys Into Illegal Gay Sex TradeColbert JohnesNessuna valutazione finora
- 365 Land Transport SafetyDocumento24 pagine365 Land Transport Safetyleo limpiasNessuna valutazione finora
- Rewire Your BrainDocumento0 pagineRewire Your BrainJohn Bates100% (1)
- Therapeutic Aquatic Exercise in The Treatment of Low Back Pain - A Systematic ReviewDocumento12 pagineTherapeutic Aquatic Exercise in The Treatment of Low Back Pain - A Systematic ReviewGleiiseTalitaNessuna valutazione finora
- Astm A 10.11Documento13 pagineAstm A 10.11edu_caneteNessuna valutazione finora
- Application For Employment Form - THPAL (2014-05) PDFDocumento7 pagineApplication For Employment Form - THPAL (2014-05) PDFRome CamingueNessuna valutazione finora
- Stepping Inside The Mind: Da Vinci and The World of The Human BrainDocumento5 pagineStepping Inside The Mind: Da Vinci and The World of The Human BrainbarakuparaNessuna valutazione finora
- 1272 PDFDocumento4 pagine1272 PDFsNessuna valutazione finora
- The Value of Urine Specific Gravity in Detecting Diabetes Insipidus in A Patient With DMDocumento2 pagineThe Value of Urine Specific Gravity in Detecting Diabetes Insipidus in A Patient With DMFaryalBalochNessuna valutazione finora
- DataFlow Application PackDocumento8 pagineDataFlow Application PackvaranasidineshNessuna valutazione finora
- Recurrent Abdominal Pain in ChildrenDocumento10 pagineRecurrent Abdominal Pain in ChildrenBariša KiršnerNessuna valutazione finora
- Self Managed TeamsDocumento13 pagineSelf Managed TeamsSiraj SiddiquiNessuna valutazione finora
- DBT Goals of Skills TrainingDocumento6 pagineDBT Goals of Skills TrainingDaniel Andres Racines JervesNessuna valutazione finora
- Formulasi Fast Desintegrating Tablet (FDT) Sari Buah Jambu Biji Merah Dengan Perbedaan Konsentrasi Ac-DisolDocumento8 pagineFormulasi Fast Desintegrating Tablet (FDT) Sari Buah Jambu Biji Merah Dengan Perbedaan Konsentrasi Ac-Disolfauzul husnaNessuna valutazione finora
- Weekly Report 13 - 19 2017Documento11 pagineWeekly Report 13 - 19 2017Sitha MahendrataNessuna valutazione finora
- Adhd Powerpoint-1Documento21 pagineAdhd Powerpoint-1api-516280936Nessuna valutazione finora
- A Detailed Lesson Plan in ScienceDocumento6 pagineA Detailed Lesson Plan in ScienceJohny Villanueva78% (72)