Potrebbero piacerti anche
- Vascular Surgery OsceDocumento66 pagineVascular Surgery Osceapi-19579909233% (3)
- Blood Supply of BrainDocumento12 pagineBlood Supply of BrainSharon Rose Genita Medez100% (1)
- Pass ProgramDocumento528 paginePass ProgramEvelyn Lee Russell67% (3)
- CP UpdatedDocumento45 pagineCP UpdatedSivakumar Kathuu KarthikeyanNessuna valutazione finora
- 1.2a Disorders of The Optic NerveDocumento7 pagine1.2a Disorders of The Optic NerveBea SamonteNessuna valutazione finora
- Neurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesDa EverandNeurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesNessuna valutazione finora
- Organic Brain SyndromeDocumento40 pagineOrganic Brain SyndromeShaz ZrinNessuna valutazione finora
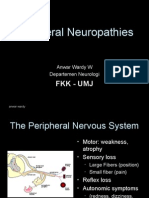
- 7 Peripheral Neuropathy MyopathyDocumento83 pagine7 Peripheral Neuropathy Myopathymuhammadridhwan100% (1)
- Nursing Lecture NeurologicalDocumento28 pagineNursing Lecture NeurologicalAedge010100% (1)
- Dementia Evaluation and TreatmentDocumento12 pagineDementia Evaluation and Treatmentrofi modiNessuna valutazione finora
- Cranial Nerve Examination Part IDocumento91 pagineCranial Nerve Examination Part IAARYA100% (1)
- Basic Overview of NeurologyDocumento45 pagineBasic Overview of NeurologyDith Rivelta CallahanthNessuna valutazione finora
- Friedreich Ataxia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandFriedreich Ataxia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Fitz Neurology Paces NotesDocumento40 pagineFitz Neurology Paces NotesDrShamshad Khan100% (1)
- Delirium and Its ManagmentDocumento64 pagineDelirium and Its ManagmentViren Solanki100% (1)
- Communication Osce 20 2 14Documento11 pagineCommunication Osce 20 2 14api-195799092Nessuna valutazione finora
- Music Therapy and MusicMedicineDocumento7 pagineMusic Therapy and MusicMedicineAnjuka100% (1)
- PolyneuropathyDocumento17 paginePolyneuropathyPraluki HerliawanNessuna valutazione finora
- Approach To Neurological DiseaseDocumento27 pagineApproach To Neurological DiseaseNEuRoLoGisT CoFFeeCuP100% (9)
- Soal Ujian Neurotrauma Full - JWBDocumento22 pagineSoal Ujian Neurotrauma Full - JWBTina HerreraNessuna valutazione finora
- Eye Movement Disorders: Professor Dr. Ayman Youssef Ezeddin EassaDocumento25 pagineEye Movement Disorders: Professor Dr. Ayman Youssef Ezeddin EassaEhab Khiry100% (1)
- DementiaDocumento40 pagineDementiakhusnulNessuna valutazione finora
- Neuro-Ophthalmology Review Authr Daniah AlshowaeirDocumento50 pagineNeuro-Ophthalmology Review Authr Daniah AlshowaeirRAJNessuna valutazione finora
- Approach Neurologic DiagnosisDocumento8 pagineApproach Neurologic DiagnosisDeepak GhimireNessuna valutazione finora
- Cognitive DisordersDocumento29 pagineCognitive DisordersKobi DabushNessuna valutazione finora
- Whiplash Injury Spondylosis, Spondolysis and SpondylolisthesisDocumento58 pagineWhiplash Injury Spondylosis, Spondolysis and SpondylolisthesistoobaNessuna valutazione finora
- Neurological Disorders: Paul Kelner, M.DDocumento97 pagineNeurological Disorders: Paul Kelner, M.DDrGasnasNessuna valutazione finora
- Organic Mental DisorderDocumento40 pagineOrganic Mental DisorderSumam NeveenNessuna valutazione finora
- 36 - Congenital Anomalies 2010Documento62 pagine36 - Congenital Anomalies 2010DARWING PADILLANessuna valutazione finora
- Idiopathic Parkinson's Disease (IPD) : A-Level Human Biology/ NursingDocumento38 pagineIdiopathic Parkinson's Disease (IPD) : A-Level Human Biology/ Nursingsarah morleyNessuna valutazione finora
- Management of Acquired Brain Injury: A Guide For Ward NursesDocumento9 pagineManagement of Acquired Brain Injury: A Guide For Ward NursesAFINANessuna valutazione finora
- Glaucoma and TinnitusDocumento20 pagineGlaucoma and Tinnitusqurat-ul-ain.sonNessuna valutazione finora
- 005 - Polyneuropathy GBSDocumento54 pagine005 - Polyneuropathy GBSLucas Victor AlmeidaNessuna valutazione finora
- Optic Disc: Symptoms of The Optic Nerve DiseasesDocumento11 pagineOptic Disc: Symptoms of The Optic Nerve DiseasesDilawar JanNessuna valutazione finora
- Cerebellar ExaminationDocumento5 pagineCerebellar ExaminationRie Aoyama-Wang100% (1)
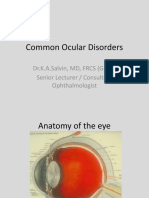
- Common Ocular DisordersDocumento108 pagineCommon Ocular DisordersKa SalvinNessuna valutazione finora
- Introduction To Neuro-Ophthalmology: Raed Behbehani, MD FRCSCDocumento50 pagineIntroduction To Neuro-Ophthalmology: Raed Behbehani, MD FRCSCMarvinson Hermogino AquinoNessuna valutazione finora
- Neurodegenerative Iand IIDocumento47 pagineNeurodegenerative Iand IIjuan carlos muñozNessuna valutazione finora
- Flashcards NeuroDocumento21 pagineFlashcards Neuroamralyamani06Nessuna valutazione finora
- Anamnesis Dan Diagnosis Topis (Dr. Hendro SP.S)Documento27 pagineAnamnesis Dan Diagnosis Topis (Dr. Hendro SP.S)PatrickNicholsNessuna valutazione finora
- Diabetic Neuropathy: DR Shahjada SelimDocumento129 pagineDiabetic Neuropathy: DR Shahjada SelimmadboyNessuna valutazione finora
- Palliative Care Delirium - DR Lesley YoungDocumento43 paginePalliative Care Delirium - DR Lesley Youngmalaysianhospicecouncil6240100% (1)
- Alzheimer's DiseaseDocumento61 pagineAlzheimer's DiseaseilalcNessuna valutazione finora
- Althimer's ResearchDocumento99 pagineAlthimer's Researchdeemoney3Nessuna valutazione finora
- Medical Approach To Dizzy PatientsDocumento52 pagineMedical Approach To Dizzy PatientsYudith Kattiarni Aisyah, MDNessuna valutazione finora
- Media 221736 enDocumento58 pagineMedia 221736 ensamNessuna valutazione finora
- History Taking in Stroke PatientDocumento23 pagineHistory Taking in Stroke PatientIndra T BudiantoNessuna valutazione finora
- Idiopathic Parkinson's Disease (IPD) : Presented By: V. Mounika Priyanka Pharm-D VTH Year 11YO1TOO17Documento37 pagineIdiopathic Parkinson's Disease (IPD) : Presented By: V. Mounika Priyanka Pharm-D VTH Year 11YO1TOO17Dr-Jagadeesh MangamooriNessuna valutazione finora
- Approach To Neurological DiseaseDocumento22 pagineApproach To Neurological DiseaseSujan ThapaNessuna valutazione finora
- 5-History Taking and Neurological ExaminationDocumento114 pagine5-History Taking and Neurological ExaminationLolla SinwarNessuna valutazione finora
- Dizziness in The Elderly: Steven Zweig, MD Family and Community Medicine MU School of MedicineDocumento34 pagineDizziness in The Elderly: Steven Zweig, MD Family and Community Medicine MU School of MedicineManish Chandra PrabhakarNessuna valutazione finora
- Cerebral Palsy (CP)Documento23 pagineCerebral Palsy (CP)Piyu ShindeNessuna valutazione finora
- DEMENTIA: Alzheimer's Disease and Vascular Dementia: Christian Kamallan NeurologistDocumento86 pagineDEMENTIA: Alzheimer's Disease and Vascular Dementia: Christian Kamallan NeurologistLuthfi HakimNessuna valutazione finora
- Mon 11-30 Neuroimaging Pearls For The Primary Care Provider - 0Documento25 pagineMon 11-30 Neuroimaging Pearls For The Primary Care Provider - 0regarskidNessuna valutazione finora
- Periferal Neuropathy 06Documento30 paginePeriferal Neuropathy 06Sa'adah Munawaroh HDNessuna valutazione finora
- 1.neuro Intro-1 UMTDocumento51 pagine1.neuro Intro-1 UMTLOVELY WALEEDNessuna valutazione finora
- Agitated Delirium 2Documento54 pagineAgitated Delirium 2Vishwa ReddyNessuna valutazione finora
- Neurological Function: Mark Ebony SumalinogDocumento51 pagineNeurological Function: Mark Ebony SumalinogAngel FiloteoNessuna valutazione finora
- Dementia: I Wayan Tunjung, DR - Sp.S. Bagian Neurologi RSU Kota MataramDocumento67 pagineDementia: I Wayan Tunjung, DR - Sp.S. Bagian Neurologi RSU Kota MataramHerlinawatiHariniNessuna valutazione finora
- Tratable DementiaDocumento100 pagineTratable Dementiaknowledgeguruos179Nessuna valutazione finora
- Multiple Sclerosis MS Demyelinating DiseaseDocumento11 pagineMultiple Sclerosis MS Demyelinating DiseaseAtie AlinaNessuna valutazione finora
- Cerebral PalsyDocumento25 pagineCerebral PalsyNandita ChatterjeeNessuna valutazione finora
- NEURO Exam and Labs, Lecture For NeuroDocumento36 pagineNEURO Exam and Labs, Lecture For NeuroNdor BariboloNessuna valutazione finora
- Lesson 9 - StrokeDocumento46 pagineLesson 9 - StrokeBetram NorascoNessuna valutazione finora
- Idiopathic Parkinson's Disease (IPD) : DR Nandita PrabhatDocumento37 pagineIdiopathic Parkinson's Disease (IPD) : DR Nandita PrabhatNandita PrabhatNessuna valutazione finora
- Rheumatologyc 2 FDocumento19 pagineRheumatologyc 2 Fapi-195799092Nessuna valutazione finora
- Neurology For FinalsDocumento90 pagineNeurology For Finalsapi-195799092Nessuna valutazione finora
- Acs Heart FailureDocumento43 pagineAcs Heart Failureapi-195799092Nessuna valutazione finora
- ArrythmiapptDocumento38 pagineArrythmiapptapi-195799092Nessuna valutazione finora
- OncologyDocumento31 pagineOncologyapi-195799092Nessuna valutazione finora
- UrologyDocumento34 pagineUrologyapi-195799092Nessuna valutazione finora
- Fluid PrescriptionDocumento1 paginaFluid Prescriptionapi-195799092Nessuna valutazione finora
- EndocrinologyDocumento37 pagineEndocrinologyapi-195799092Nessuna valutazione finora
- Haematology TransfusionsDocumento28 pagineHaematology Transfusionsapi-195799092Nessuna valutazione finora
- Station 7 Blood TransfusionDocumento5 pagineStation 7 Blood Transfusionapi-195799092Nessuna valutazione finora
- Station 8 DnacprDocumento6 pagineStation 8 Dnacprapi-195799092Nessuna valutazione finora
- Station 9 AbdoDocumento7 pagineStation 9 Abdoapi-195799092Nessuna valutazione finora
- Station 10 AnaphylaxisDocumento7 pagineStation 10 Anaphylaxisapi-195799092Nessuna valutazione finora
- Station 5 NeuroDocumento8 pagineStation 5 Neuroapi-195799092Nessuna valutazione finora
- Station 6 EndocrineDocumento6 pagineStation 6 Endocrineapi-195799092Nessuna valutazione finora
- Data InterpretationDocumento79 pagineData Interpretationapi-195799092Nessuna valutazione finora
- Ear Nose and Throat 2Documento34 pagineEar Nose and Throat 2api-195799092Nessuna valutazione finora
- Station 2 Drug ErrorDocumento5 pagineStation 2 Drug Errorapi-195799092Nessuna valutazione finora
- Station 4 RespDocumento6 pagineStation 4 Respapi-195799092Nessuna valutazione finora
- Station 3 AkiDocumento6 pagineStation 3 Akiapi-195799092Nessuna valutazione finora
- Station 1 CardioDocumento6 pagineStation 1 Cardioapi-195799092Nessuna valutazione finora
- Infectious DiseasesDocumento22 pagineInfectious Diseasesapi-195799092Nessuna valutazione finora
- Asthma Copd AnaphylaxisDocumento35 pagineAsthma Copd Anaphylaxisapi-195799092Nessuna valutazione finora
- Trauma and Orthopaedics 11 2 14Documento21 pagineTrauma and Orthopaedics 11 2 14api-195799092Nessuna valutazione finora
- Gastroexamination FDocumento43 pagineGastroexamination Fapi-195799092Nessuna valutazione finora
- Rheumatology Presentation To SendDocumento92 pagineRheumatology Presentation To Sendapi-195799092Nessuna valutazione finora
- Vascular Surgery 4 2 14Documento35 pagineVascular Surgery 4 2 14api-195799092Nessuna valutazione finora
- Medical and Surgical Emergencies Karen BallDocumento62 pagineMedical and Surgical Emergencies Karen Ballapi-195799092Nessuna valutazione finora
- Shock Sepsis c2f Recorded VersionDocumento45 pagineShock Sepsis c2f Recorded Versionapi-195799092Nessuna valutazione finora
- IBPS PO Memory Based Test (Shift 3) - 4th Dec 2021 EnglishDocumento28 pagineIBPS PO Memory Based Test (Shift 3) - 4th Dec 2021 EnglishPranjal ArgalNessuna valutazione finora
- Biology Investigatory Project Class 12thDocumento20 pagineBiology Investigatory Project Class 12thsupercelldarshil100% (1)
- Seminar CNE 2018Documento12 pagineSeminar CNE 2018Aan Dwi PrasetioNessuna valutazione finora
- Masdar Muid Lab/SMF. Ilmu Kesehatan Anak FK. Unibraw / RSU Dr. Saiful Anwar MalangDocumento7 pagineMasdar Muid Lab/SMF. Ilmu Kesehatan Anak FK. Unibraw / RSU Dr. Saiful Anwar MalangputriNessuna valutazione finora
- Role of NeuropsychologistDocumento15 pagineRole of NeuropsychologistMahnoor MalikNessuna valutazione finora
- Carlos Herraiz - HYPERACUSISDocumento45 pagineCarlos Herraiz - HYPERACUSISavalon_moonNessuna valutazione finora
- CHAPTER 2 Science Form 4Documento59 pagineCHAPTER 2 Science Form 4Lopak TikeNessuna valutazione finora
- 2015 Movement DisordersDocumento567 pagine2015 Movement DisordersAndreea Raluca CimpoiNessuna valutazione finora
- Evaluation and Management of Elevated Intracranial Pressure in Adults - UpToDateDocumento41 pagineEvaluation and Management of Elevated Intracranial Pressure in Adults - UpToDateManuelEduardoSanchezSotoNessuna valutazione finora
- Faktor PICODocumento1 paginaFaktor PICOAlldo SaodalaNessuna valutazione finora
- Ataxia: Dr. Vipinnath E.N. (PT)Documento18 pagineAtaxia: Dr. Vipinnath E.N. (PT)AKHILNessuna valutazione finora
- Curriculum Vitae Rima Chaudhari 14042021Documento8 pagineCurriculum Vitae Rima Chaudhari 14042021meenakshi.r.agrawalNessuna valutazione finora
- DR Bashir Ahmed Dar Associate Professor Medicine Chinkipora Sopore KashmirDocumento23 pagineDR Bashir Ahmed Dar Associate Professor Medicine Chinkipora Sopore KashmiranandtmcNessuna valutazione finora
- Types of Ques-McqDocumento8 pagineTypes of Ques-Mcqsheetal taneja100% (2)
- 1 - Cranial Nerve 5, 6,7Documento44 pagine1 - Cranial Nerve 5, 6,7ewijayapalaNessuna valutazione finora
- ASIADocumento2 pagineASIALuis Galván BastidasNessuna valutazione finora
- Overview of Health Facility Planning in MOH - DR - Saudah PDFDocumento26 pagineOverview of Health Facility Planning in MOH - DR - Saudah PDFtarmiziNessuna valutazione finora
- Web Osseo ProgramDocumento6 pagineWeb Osseo Programav1986362Nessuna valutazione finora
- Epilepsy and Brain LesionDocumento9 pagineEpilepsy and Brain LesionPosadasLoezaJosueKarlaNessuna valutazione finora
- Nur6501 Week 8 Assignment 2 The Pathophysiology of Disorders PDFDocumento3 pagineNur6501 Week 8 Assignment 2 The Pathophysiology of Disorders PDFtutor12345Nessuna valutazione finora
- Lumbar PunctureDocumento6 pagineLumbar PunctureMitkoNessuna valutazione finora
- Tuberculous MeningitisDocumento11 pagineTuberculous MeningitiszuhriNessuna valutazione finora
- Camillo Negro and His Contributions To NeurologyDocumento3 pagineCamillo Negro and His Contributions To NeurologyPsikiatri 76 UndipNessuna valutazione finora
- Articles: BackgroundDocumento11 pagineArticles: BackgroundricardojosesotofontalvoNessuna valutazione finora
- Otitis MediaDocumento98 pagineOtitis MediaLody Lean CruzNessuna valutazione finora
- Psychiatric and Behavioral Aspects of Epilepsy Current Perspectives and MechanismsDocumento484 paginePsychiatric and Behavioral Aspects of Epilepsy Current Perspectives and MechanismsTanvi GuptaNessuna valutazione finora